
Data Availability Statement
Deidentified data supporting the findings of this study are available from the corresponding author upon reasonable request.
Funding Information
The authors would like to thank Khalid and Kholoud Al Thani for their support they have provided for the New England Center for Children’s Early Markers of Autism Project.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (IRB) at Western New England University. Written informed consent and release documents were obtained from the child’s legal guardians. Child assent was continuously monitored throughout the study.
Abstract
Both neurobiological and behavioral indicators of autism spectrum disorder (ASD) have been described in the first year of life; however, many children experience significant delays in accessing services. Identifying the earliest signs of ASD provides the opportunity to preemptively intervene and improve outcomes. This longitudinal case study documents the emergence of prodromal signs of ASD and the implementation of a novel preemptive intervention model beginning at 8 weeks old. The participant was enrolled through a specialized research and educational facility in the United States. Prodromal ASD behaviors at 8 weeks included eye gaze avoidance, reduced orienting to sound, and diminished social smiling. Intervention followed a scaffolded model of parent coaching and naturalistic, developmentally-informed behavioral therapy. At 12 months, the participant met ASD diagnostic criteria and began receiving intensive one-to-one therapy. Observational and standardized assessment data showed skill gains throughout the course of intervention, with the most substantial progress during intensive therapy. By age 2, the participant no longer met ASD diagnostic criteria, and developmental gains were maintained at 5 years. This case study details ASD symptom progression, presents a framework for a scaffolded preemptive intervention, and provides additional support for intensive, developmentally-informed behavioral interventions in achieving optimal outcomes.
Keywords: Autism Spectrum Disorder, early identification, parent coaching, early intervention, high-risk infants
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by impairments in social communication and restricted, repetitive behavior (American Psychiatric Association [APA], 2013). Neurobiological and behavioral indicators of ASD have been documented in the first year (Courchesne et al., 2019). Despite early signs, diagnosis remains unreliable until complex social behaviors emerge (Pierce et al., 2019). Early identification improves access to services and quality of life, yet most children are not diagnosed before age 4 (Maenner et al., 2021). Identifying early markers allows for intervention before ASD fully manifests, but consensus on their timing and presentation varies, and few studies have explored infant intervention models (Ozonoff et al., 2018; Rogers et al., 2014).
While the predictive validity of ASD indicators before 12 months is unclear, research supports the emergence of prodromal behaviors in the first year (Ozonoff et al., 2018; Zwaigenbaum et al., 2021). Studies report differences in social and nonsocial attention as early as 1 week (Di Giorgio et al., 2016), reduced eye contact by 2 months (Bradshaw et al., 2020; Gangi et al., 2021; Jones & Klin, 2013), and diminished responsiveness to social cues by 6 months (Chawarska et al., 2013). Broader attention differences and atypical crying patterns have also been noted (Elsabbagh et al., 2013; Sheinkopf et al., 2012). Research further indicates reduced sensitivity to social stimuli between 6 and 12 months (Macari et al., 2021) and inconsistent response to joint attention by 9 months (Stallworthy et al., 2022). Motor delays, including poor coordination, head lag, and postural instability, have been observed from 3 months (Libertus et al., 2014), with repetitive behaviors documented by 8 months (Scully et al., 2023).
Early identification enables timely interventions and improved outcomes. Applied Behavior Analysis (ABA) is a widely accepted, evidence-based ASD intervention (Vismara & Rogers, 2010). Earlier diagnosis has led to developmentally-informed models like Naturalistic Developmental Behavioral Interventions (NDBIs) which integrate behavioral strategies into daily routines with caregiver involvement (Schreibman et al., 2015). Early Intensive Behavioral Intervention (EIBI) is another well-supported approach, emphasizing systematic instruction and one-on-one support, yielding lasting gains in language, cognition, and social skills (MacDonald et al., 2014).
Despite evidence of early ASD signs, few interventions target infants under 12 months. Rogers et al. (2014) adapted the Early Start Denver Model (ESDM) for infants 9–15 months, showing reduced ASD onset by 36 months. Colombi et al. (2023) extended these findings to a 6-month-old, who later developed typically.
ASD behaviors are detectable before 12 months, but preemptive interventions before 6 months remain unexplored. This case study documents ASD symptom emergence in a high-risk infant from 2 months and extends EIBI and NDBI research by presenting a novel early intervention.
Methods
Mark was an 8-week-old male infant enrolled in the ongoing Infant Sibling Study at the New England Center for Children (NECC). His family was White and English was the only language spoken by his family. He had two older brothers with ASD, but no other relevant family history. Mark was born full-term after an uncomplicated pregnancy and delivery. His Apgar score was normal, and he was deemed healthy at birth. After developmental concerns emerged at 8 weeks, Mark was referred for medical follow-up. At 3 months, he underwent audiological testing and an early intervention evaluation. Hearing was normal, but he qualified for early intervention due to cognitive and motor delays.
At 4 months, Mark’s pediatrician noted an increase in head circumference from the 75th to the 100th percentile. An ultrasound showed no neurological abnormalities. Before 12 months, Mark had recurring ear infections and received tympanostomy tubes. Follow-up audiological testing was normal. At 12 months, Mark attended a neurodevelopmental evaluation at a specialized autism clinic. A licensed psychologist outside NECC determined he met diagnostic criteria for ASD.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (IRB) at Western New England University. Written informed consent and release documents were obtained from the child’s legal guardians. Child assent was continuously monitored throughout the study.
Intervention
The intervention was delivered using a scaffolded model that included parent coaching alone, parent coaching with 15 hours of one-to-one therapy per week, and parent coaching with 30 hours of one-to-one therapy per week (see Table 1).
Table 1. Overview of Intervention Components.
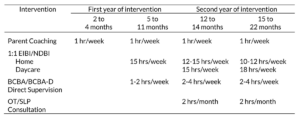
Behavioral Intervention; BCBA= Board-Certified Behavior Analyst (master’s level); BCBA-D=
Doctoral-Level Board-Certified Behavior Analyst; OT= Occupational Therapist; SLP= Speech
and Language Pathologist.
Parent Coaching
Parent coaching sessions were held at home for one hour weekly. Sessions were primarily with Mark’s mother, though other family members, including siblings, participated. Coaching involved collaborative engagement, individualized goals, and structured family activities to support skill development. Each session began with a check-in to provide support, answer questions, and identify needs. Throughout sessions, the therapist provided psychoeducation, including strategies to foster skills through imitation and praise, maximizing enjoyment in social exchanges, and sustaining positive joint interactions. The therapist demonstrated activities, modeled approaches, and observed the parent practice each skill with Mark before providing feedback. Sessions concluded with discussing how to incorporate practice into daily routines (e.g., diaper changing, bathtime). The approach encouraged family involvement and was adapted to individual needs.
One-to-One Therapy
One-to-one therapy integrated principles from established NDBI and EIBI models. Interventions were embedded within daily routines, used natural consequences, and incorporated Mark’s interests to promote motivation and engagement. Learning opportunities were created by following Mark’s lead and structuring the environment to support skill development through strategies such as playful obstruction, controlled toy access, and adult-led social activities (e.g., blowing bubbles, pushing a swing). Skills were broken into smaller steps, and acquisition was supported through modeling, maximizing opportunities for success, and repeated practice. A primary goal was to foster independence in natural settings. Therapist support was systematically faded, and skills demonstrated in one-to-one therapy were incorporated into parent coaching sessions to support generalization across contexts with family members.
Staffing
Parent-coaching sessions and standardized assessment batteries were conducted by a licensed clinical psychologist and doctoral-level Board Certified Behavior Analyst (BCBA). One-to-one interventions were delivered by trained therapists enrolled in an ABA master’s program. In-person one-to-one therapy supervision occurred weekly by either the overseeing psychologist or a master’s-level BCBA. Weekly team meetings were held to monitor Mark’s response to intervention and adjust therapy goals as needed. Beginning at 12 months old, a doctoral-level speech-language pathologist and a master’s-level occupational therapist provided monthly consultation through Mark’s home-based EIBI program.
Curriculum
A developmental scope and sequence was established for each skill domain (e.g., cognitive, social-emotional, fine motor, gross motor, communication) to guide therapy goals and intervention planning. Skills were selected and arranged using research on patterns of social and regulatory behavior in infancy, criterion-referenced milestone norms, and existing curriculum systems for at-risk infants and young children (Johnson-Martin et al., 2004; Nugent et al., 2007, Sheldrick et al., 2019; Squires et al., 2009). As the intervention progressed, published interventions for toddlers with ASD (e.g., ESDM, EIBI) informed social skill goals. Intervention targets were introduced systematically and selected based on Mark’s developmental level and chronological age. A hierarchical model of skill development was used, with an emphasis on developing foundational skills before introducing more advanced abilities. Curriculum guides were developed for each skill and specified how to create learning opportunities, facilitate responding, and provide natural consequences to establish each skill. Figure 1 depicts the progression of curriculum targets throughout the intervention.
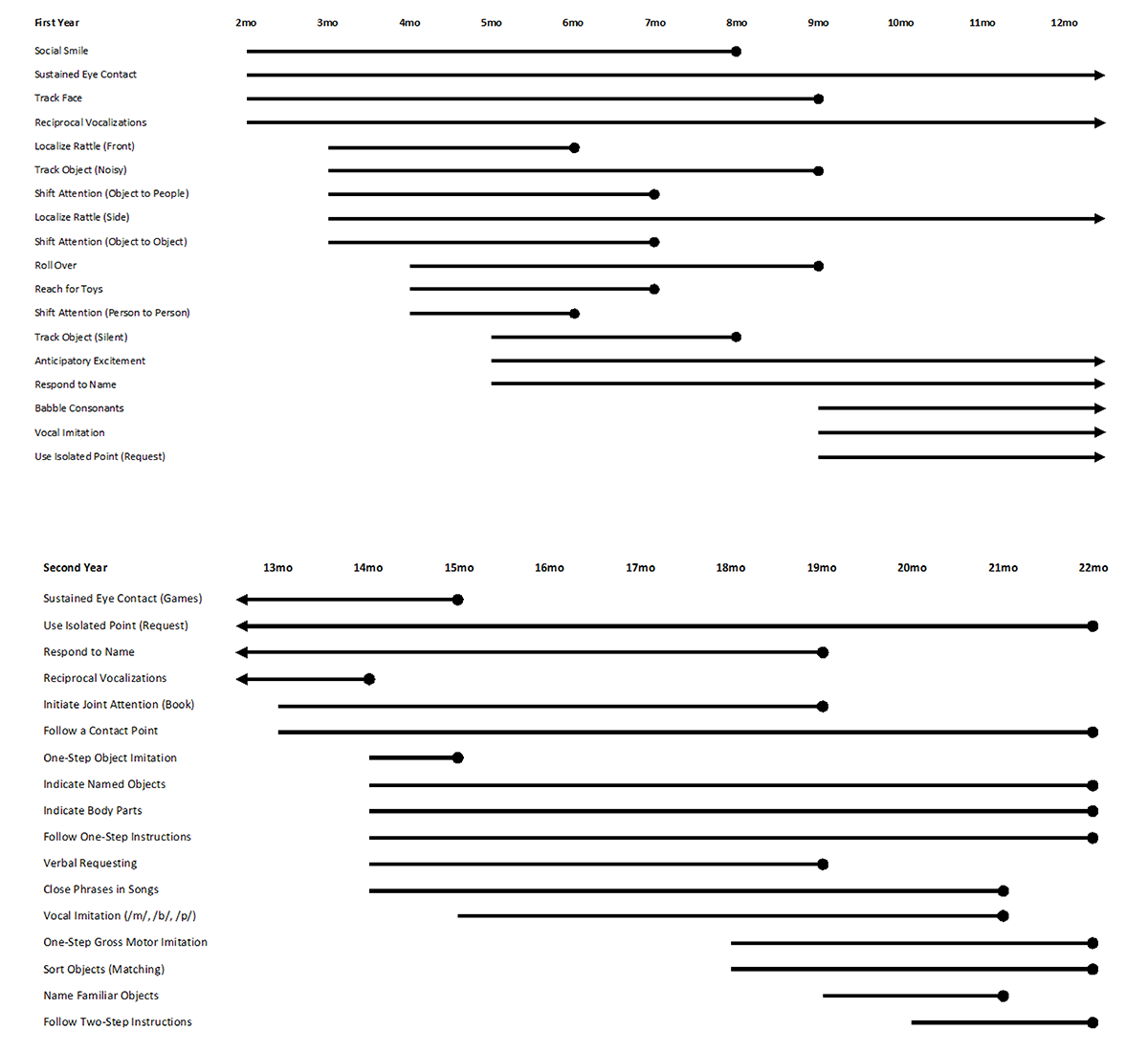
Note. This figure demonstrates the progression of curriculum targets across the first and second years of life. Mark’s age in months is reflected in the top panel of the diagrams. Each horizontal line indicates a target skill in intervention and begins at the age in which the skill was introduced. Arrows reflect skills that were targeted across both the first and second years of life. Solid circles indicate mastery of a target skill. Skills are listed in the order in which they were taught.
First Year of Life
2 through 4 months
Clinicians first noted developmental concern during Mark’s initial evaluative session at 8 weeks old. He displayed a flat affect, gaze avoidance, reduced visual tracking, and diminished orientation to sound (e.g., his mother’s voice). Parent coaching was initiated, and target skills included social smiling, sustained eye contact, tracking a face, and reciprocal vocalizations. Activities were arranged to encourage social interactions and active responding through body positioning rather than physical prompting. For example, gaze avoidance was addressed by holding Mark in a cradled position and positioning the adult’s face 12 inches from midline while talking softly. Affective behavior (e.g., social smiling) was addressed similarly and began by touching Mark gently and tickling him while singing, making silly sounds, and smiling. By 3 months old, additional activities were introduced including tracking noisy objects and shifting attention between objects and people. At 4 months, parent coaching curriculum included rolling over, reaching for toys, and shifting social attention.
5 through 11 months
At 5 months of age, Mark began receiving 15 hours per week of one-to-one therapy. Targets included tracking silent objects, responding to his name with eye contact, and displaying anticipatory excitement during games. By 6 months old, Mark independently localized a rattle at midline and shifted attention between familiar adults. At 7 months, Mark began gaze shifting between objects and people and started reaching for toys. Social smiling and tracking a silent object were mastered by 8 months old.
By 9 months, Mark began visually tracking objects/people and started rolling. At that time, intervention focused on increasing vocalizations and using an isolated finger point. At 10 months, Mark began displaying emerging repetitive behavior mannerisms. He began repeatedly patting toys with an open palm or finger and a reduction in developmentally-appropriate object exploration was observed. As these behaviors inhibited Mark’s ability to develop other foundational skills, more appropriate toy play became a target of intervention. The therapist neutrally redirected repetitive engagement by introducing close-ended construction activities and modeling appropriate engagement. By 11 months, Mark had made gains in gross motor progression (e.g., crawling); however, repetitive behavior and delays in communicative and social development remained.
Second Year of Life
12 through 14 months
At 12 months old, Mark received a formal ASD diagnosis and was enrolled in a home-based EIBI program for 25 to 30 hours per week. Target skills remained developmentally-informed and therapy sessions accommodated Mark’s nap schedule and daily routines. Skills introduced during the first year of intervention were targeted in sessions until independence was achieved. An overarching goal was to develop skills to ensure success in an integrated setting without one-to-one support. Mark began attending a community daycare two days per week with a therapist. Mark was placed in a classroom with eight typically-developing, age-matched peers. Skills that were not observed in daycare were taught during home-based sessions or through least-intrusive supports provided by the therapist in the classroom. Between 13 and 14 months of age, curriculum targets included sustained eye contact during games (e.g., turn-taking with a ball), responding to and initiating joint attention, receptive language (e.g., following instructions, indicating body parts), expressive language, and parallel and constructive play.
15 through 22 months
Between the ages of 15 and 22 months, one-to-one therapy, parent-coaching, and routine developmental evaluations continued. Daycare hours increased to two and a half days per week. At 15 months, Mark began engaging in sustained eye contact during games and started to independently imitate one-step actions with objects. At 18 months, targets included imitating motor actions, matching and sorting objects within a classroom cleanup routine, naming objects, and following two-step instructions. Between 19 and 21 months, significant skill gains were observed across communicative and social domains. Mark began independently responding to his name, spontaneously initiating joint attention, naming objects, making requests, and completing simple phrases when singing songs. By 22 months, Mark used an isolated point to request, responded to bids for joint attention, indicated objects and body parts, followed multi-step directions, imitated actions, and sorted toys. Therapist support was gradually faded across settings and services were discontinued.
Outcome Measures
Mark’s developmental progress was assessed weekly through his performance on systematic, criterion-referenced assessment instruments and structured observations based on age-normed items from milestone questionnaires (Harden & Peisner-Feinberg, 2001; Squires et al., 2009). Beginning at 6 months, comprehensive neurodevelopmental batteries were completed every 3 months to assess social, cognitive, adaptive, communication, and motor progression using standardized assessments.
Mullen Scales of Early Learning (MSEL; Mullen, 1995)
The MSEL is a standardized assessment designed for use with children from birth to 68 months of age. Performance is measured across five domains, including Visual Reception, Fine Motor, Receptive Language, Expressive Language, and Gross Motor. The MSEL has strong internal consistency and test-retest reliability (Mullen, 1995). The MSEL was administered at 6, 12, 15, 18, 22, 34, and 38 months of age.
Autism Observation Scale for Infants (AOSI; Bryson et al., 2008)
The AOSI is a semi-structured measure designed to detect and monitor for early signs of autism in infant siblings ages 6 to 18 months of age. It consists of six behavioral presses during which social communicative behaviors (e.g., eye contact, orientation to name, social smiling) and non-social communication behaviors (e.g., disengagement of attention, repetitive behaviors) are assessed. The AOSI has strong interrater reliability and fair test-retest stability (Bryson et al., 2008). The AOSI was administered at 6, 12, 15, and 18 months of age.
Autism Diagnostic Observation Schedule, Second Edition (ADOS- 2; Lord et al., 2012)
The ADOS-2 is a standardized measure designed to elicit social and communicative behaviors and assess for symptoms associated with an autism spectrum disorder. Administration occurs through a series of structured and unstructured activities that allow for a direct observation of behavior. The presented activities and scoring algorithm are dependent on the individual’s chronological age and language abilities. Performance on the ADOS-2 is depicted as range of concern for an autism spectrum disorder or a diagnostic classification (Lord et al., 2012). The ADOS-2 was administered at 12, 15, 18, 22, and 38 months of age.
Vineland Adaptive Behavior Scales, Third Edition (VABS-3; Sparrow et al., 2016)
The VABS-3 is a semi-structured parent interview designed for use with individuals from birth to 90 years. Performance is measured across Communication, Daily Living, Socialization, and Motor adaptive skill domains that comprise an Adaptive Behavior Composite. The VABS-3 has strong internal consistency and test-retest reliability (Sparrow et al., 2016). Mark’s mother was interviewed using the VABS-3 when he was 12, 49, and 62 months of age.
Results
Mark initially showed delays at 2 months old, and progress was recorded through weekly milestone tracking from 2 to 24 months (see Figure 2). More formal progress tracking was completed through standardized assessments beginning at 6 months of age (see Table 2).
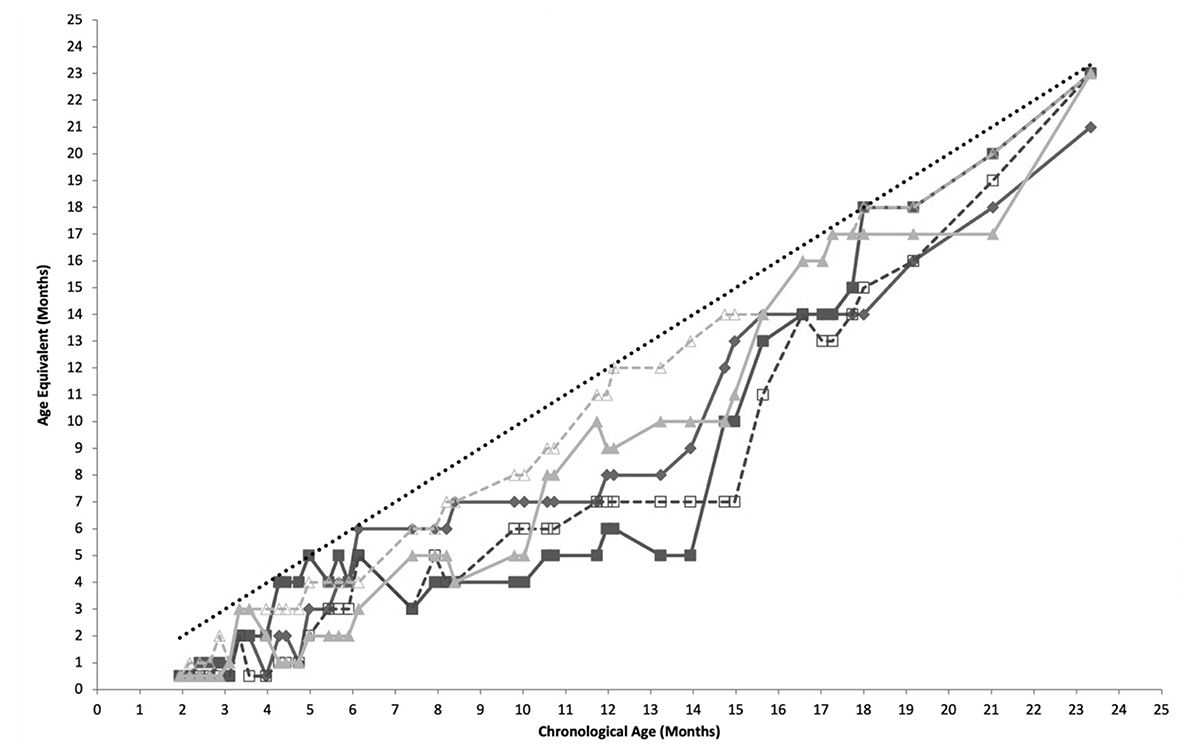
Note. Mark’s performance on weekly milestone assessments from 2 months to 24 months. EL= Expressive Language; RL= Receptive Language; AE= Age Equivalent. The dotted line represents age-level performance.
Table 2. Standardized Assessment Results.
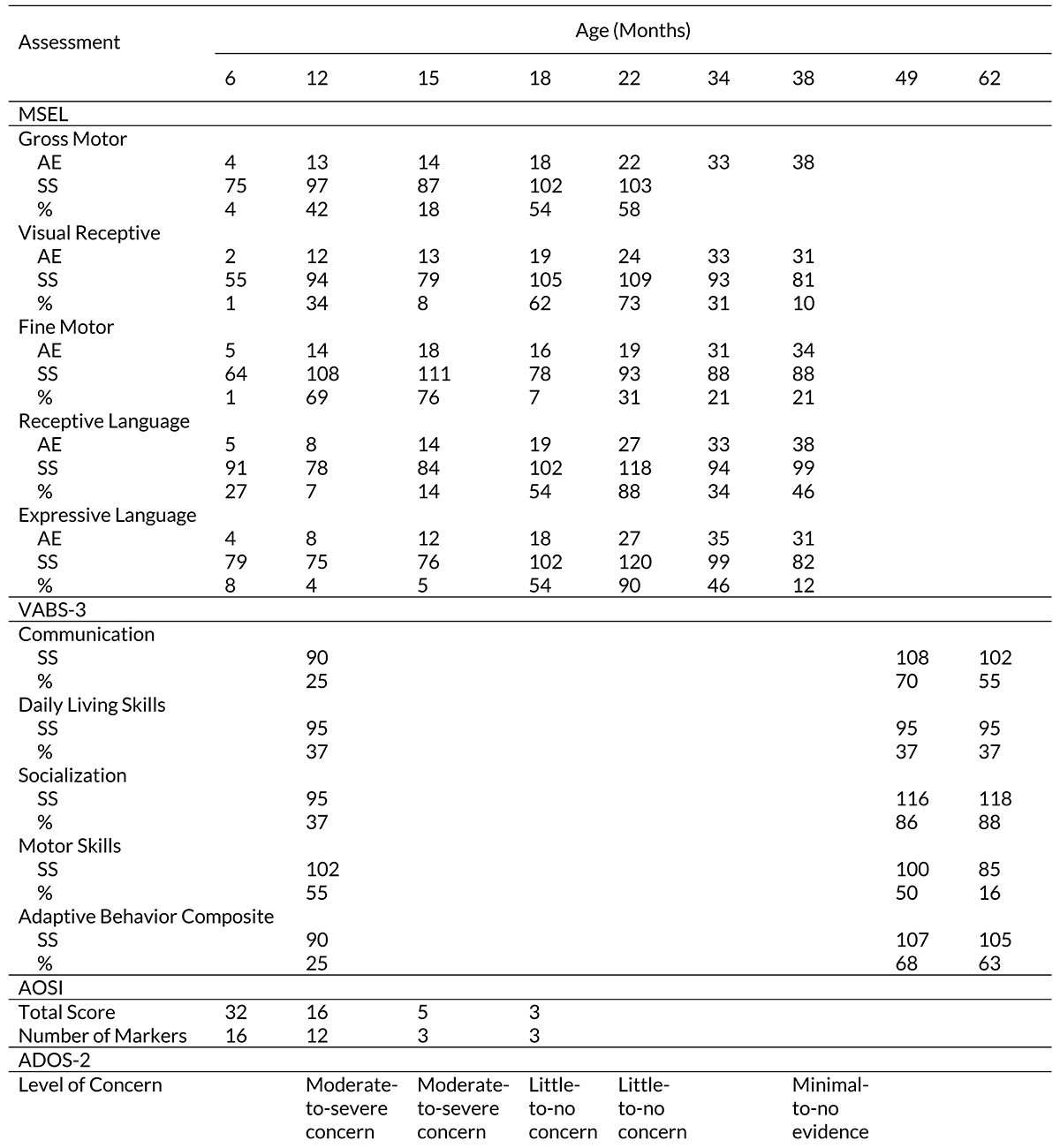
Standardized Assessment Results
At 6 months, Mark’s performance on the MSEL fell 1- to 4-months below age-level across domains. Scores in gross motor, visual reception, fine motor, and expressive language domains were substantially delayed. On the AOSI, Mark received a total score of 32 with 16 markers including reduced visual tracking, lack of orientation to name, inhibited social response, and reduced reciprocal babbling. At 12 months, Mark received a comprehensive battery of assessments including the MSEL, AOSI, ADOS-2, and VABS-3. The VABS-3 and the ADOS-2 were administered by a licensed psychologist unaffiliated with the present study. On the MSEL, average performance was observed in gross motor, visual reception, and fine motor domains with below age-level performance in areas of receptive and expressive language. Responses on the VABS-3 also supported concern in communication domains. Scores on the AOSI fell above the cutoff for ASD-risk with a total score of 16 and performance on the ADOS-2 reflected moderate-to-severe concern for ASD.
At 15 months, Mark’s performance on the MSEL fell below average in areas of visual reception, receptive language, and expressive language. Scores on the AOSI were above the threshold for ASD while performance on the ADOS-2 continued to reflect moderate-to-severe concern for ASD. At 18 months old, scores on the MSEL improved across gross motor, visual reception, receptive language, and expressive language while a reduction was observed in fine motor skills. Performance on the AOSI fell below the ASD cutoff and scores on the ADOS-2 reflected little-to-no concern for ASD. At 22 months, stable performance was observed in gross motor and visual reception domains on the MSEL while improvement occurred across fine motor, receptive language, and expressive language domains. Observation during the ADOS-2 continued to reflect little-to-no concern for ASD and one-to-one services were discontinued.
Follow-up
At 23 months old, Mark was enrolled in an integrated preschool setting without support or ancillary services. Prior to his third birthday, Mark obtained an evaluation by his public school district to determine eligibility for an Individualized Education Program. Mark did not qualify for special education services due to age-level or above performance on school-based testing.
At 34 months, Mark received initial developmental follow-up through the Infant Sibling Study. Scores on standardized measures continued to fall in the average range. Subsequent follow-up completed at 38 months revealed stability in receptive language, fine motor, and gross motor abilities. Reduced performance was observed in expressive language and visual reception domains. Performance on the ADOS-2 did not reach the cutoff for ASD and no social concerns were observed or identified during the evaluation. Additional follow-up sessions were completed when Mark was 49 and 62 months old. Results of the VABS-3 reflected average performance across communication, daily living, socialization, and motor domains. Mark is presently enrolled in a fully integrated public-school classroom and there are no reported developmental concerns.
Discussion
This case study extends the literature on early ASD signs and describes a novel intervention model for an infant showing behavioral indicators. Concerns were identified at 2 months and paralleled existing research on early ASD markers (Di Giorgio et al., 2016; Gangi et al., 2021; Jones & Klin, 2013). Intervention began at 8 weeks using a scaffolded parent coaching model and developmentally informed instruction. Targets were based on developmental literature and age norms. Response to intervention was monitored through behavioral data, milestone evaluations, and standardized assessments. After an ASD diagnosis at 12 months, additional services were provided. By age 2, Mark no longer met ASD diagnostic criteria, with maintained social skill gains.
This study documented prodromal ASD behaviors emerging at 8 weeks in a high-risk infant. Infants are born with regulatory skills, responsivity to stimuli, and motor control (Nugent, 2007), which set the foundation for social development. Research has shown atypical attention patterns (Di Giorgio et al., 2016; Elsabbagh et al., 2013), reduced eye gaze (Gangi et al., 2021; Jones & Klin, 2013), atypical vocalizations (Paul et al., 2011; Sheinkopf et al., 2012), and motor delays (Libertus et al., 2014). Delays in these areas, along with reduced affective responding, were observed in this study.
Prodromal ASD behaviors before 6 months have not been distinguished from other developmental conditions. Infant sibling research suggests ASD-specific symptoms emerge between 6 and 12 months (Ozonoff et al., 2018; Zwaigenbaum et al., 2021). However, given the accumulative nature of ASD symptoms, behaviors in early infancy likely indicate later manifestation. Between 6 and 12 months, Mark showed attentional weaknesses (e.g., inhibited disengagement, differences in social/nonsocial attention), no response to name, reduced joint attention, and emerging repetitive behaviors.
Early identification allows for timely intervention. Few interventions target the first year, and this study used a scaffolded approach to ensure developmental appropriateness. Targets addressed early skill deficits before advancing. Naturalistic behavioral principles were applied and adjusted based on developmental level. Initially, body positioning and shaping promoted responding, later progressing to modeling and proximity fading. Sessions occurred at home, embedded in daily routines (e.g., diaper changing, bath time), later expanding to daycare to encourage peer interactions.
Skill gains directly corresponded to intervention intensity. Parent coaching alone was insufficient; intensive instruction was required. Moderate gains were seen with 15 weekly intervention hours, but ASD-specific deficits remained. At 12 months, Mark received a formal ASD diagnosis, making him eligible for 30 weekly one-to-one hours, ancillary services, and increased supervision. When intervention met EIBI-supported levels (at least 28 hours/week; MacDonald et al., 2014), significant developmental progress occurred. By 22 months, Mark no longer met ASD diagnostic criteria and functioned independently in an integrated setting.
While parent coaching alone did not result in significant skill gains, this element of treatment was integral in both providing the family with support and strengthening the relationship between Mark and his mother. The present intervention incorporated parent coaching and feedback throughout the interventions to support family-based goals. This element further provided the opportunity for Mark to practice skills targeted in sessions across the day and with a number of family members. His siblings were involved, when possible, to increase opportunities for family-based care and support.
This case study documents early ASD signs and an intervention model for a high-risk infant but is limited by its single-case design. Without experimental control, external validity is reduced, and rigorous trials are needed to confirm efficacy. However, this study aligns with existing research on early ASD markers and adapts EIBI and NDBI for infants. Results suggest that identifying early developmental deviations may enhance understanding of ASD emergence, leading to earlier identification and preemptive intervention.
Currently, an ASD diagnosis is required to access services, though reliable diagnosis before 12 months is not feasible (Pierce et al., 2019). While preemptive intervention models show promise, widespread implementation is limited within existing systems. This study supports universal screening, continued research on ASD predictive markers, and randomized controlled trials on preemptive interventions (Colombi et al., 2023; Rogers et al., 2014).
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Bradshaw, J., Klin, A., Evans, L., Klaiman, C., Saulnier, C., & McCracken, C. (2020). Development of attention from birth to 5 months in infants at risk for autism spectrum disorder. Development and psychopathology, 32(2), 491-501.
Bryson, S. E., Zwaigenbaum, L., McDermott, C., Rombough, V., & Brian, J. (2008). The Autism Observation Scale for Infants: scale development and reliability data. Journal of autism and developmental disorders, 38, 731-738.
Chawarska, K., Macari, S., & Shic, F. (2013). Decreased spontaneous attention to social scenes in 6-month-old infants later diagnosed with autism spectrum disorders. Biological psychiatry, 74(3), 195-203.
Colombi, C., Chericoni, N., Bargagna, S., Costanzo, V., … & Contaldo, A. (2023). Case report: Preemptive intervention for an infant with early signs of autism spectrum disorder during the first year of life. Frontiers in Psychiatry, 14, 1105253.
Courchesne, E., Pramparo, T., Gazestani, V. H., Lombardo, M. V., Pierce, K., & Lewis, N. E. (2019). The ASD Living Biology: from cell proliferation to clinical phenotype. Molecular psychiatry, 24(1), 88-107.
Di Giorgio, E., Frasnelli, E., Rosa Salva, O., Luisa Scattoni, M., … & Vallortigara, G. (2016). Difference in visual social predispositions between newborns at low-and high-risk for autism. Scientific reports, 6(1), 26395.
Elsabbagh, M., Fernandes, J., Webb, S. J., Dawson, G., Charman, T., Johnson, M. H., & BASIS Team. (2013). Disengagement of visual attention in infancy is associated with emerging autism in toddlerhood. Biological psychiatry, 74(3), 189-194.
Gangi, D. N., Boterberg, S., Schwichtenberg, A. J., Solis, E., … & Ozonoff, S. (2021). Declining gaze to faces in infants developing autism spectrum disorder: evidence from two independent cohorts. Child development, 92(3), e285-e295.
Hardin, B. J., & Peisner-Feinberg, E. S. (2001). The Early Learning Accomplishment Profile (E-LAP). Kaplan Press, Lewisville, NC 27023-0609
Johnson-Martin, N., Attermeier, S. M., & Hacker, B. J. (2004). The Carolina curriculum for infants and toddlers with special needs. Baltimore: Paul H. Brookes.
Jones, E. J., Gliga, T., Bedford, R., Charman, T., & Johnson, M. H. (2014). Developmental pathways to autism: a review of prospective studies of infants at risk. Neuroscience & Biobehavioral Reviews, 39, 1-33.
Jones, W., & Klin, A. (2013). Attention to eyes is present but in decline in 2–6-month-old infants later diagnosed with autism. Nature, 504(7480), 427-431.
Libertus, K., Sheperd, K. A., Ross, S. W., & Landa, R. J. (2014). Limited fine motor and grasping skills in 6‐month‐old infants at high risk for autism. Child development, 85(6), 2218-2231.
Lord, C., Rutter, M., Dilavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism Diagnostic Observation Schedule, Second Edition (ADOS-2). Torrance, CA: Western Psychological Services.
Macari, S., Milgramm, A., Reed, J., Shic, F., Powell, K. K., Macris, D., & Chawarska, K. (2021). Context-specific dyadic attention vulnerabilities during the first year in infants later developing autism spectrum disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 60(1), 166-175.
MacDonald, R., Parry-Cruwys, D., Dupere, S., & Ahearn, W. (2014). Assessing progress and outcome of early intensive behavioral intervention for toddlers with autism. Research in developmental disabilities, 35(12), 3632-3644.
Maenner, M. J., Shaw, K. A., Bakian, A. V., Bilder, D. A., Durkin, M … & Cogswell, M. E. (2021). Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2018. MMWR Surveillance Summaries, 70(11), 1.
Mullen, E. M. (1995). Mullen Scales of Early Learning. Circle Pines, MN: AGS.
Nugent, J. K., Keefer, C. H., Minear, S., Johnson, L. C., & Blanchard, Y. (2007). The newborn behavioral observations (NBO) system handbook. Paul H Brookes Publishing, Baltimore, MD, USA.
Ozonoff, S., Gangi, D., Hanzel, E. P., Hill, A., Hill, M. M., Miller, M., … & Iosif, A. M. (2018). Onset patterns in autism: Variation across informants, methods, and timing. Autism Research, 11(5), 788-797.
Pierce, K., Gazestani, V. H., Bacon, E., Barnes, C. C., Cha, D., Nalabolu, S., … & Courchesne, E. (2019). Evaluation of the diagnostic stability of the early autism spectrum disorder phenotype in the general population starting at 12 months. JAMA pediatrics, 173(6), 578-587.
Rogers, S. J., & Dawson, G. (2020). Early Start Denver Model for young children with autism: Promoting language, learning, and engagement. Guilford Publications.
Rogers, S. J., Vismara, L., Wagner, A. L., McCormick, C., Young, G., & Ozonoff, S. (2014). Autism treatment in the first year of life: a pilot study of infant start. Journal of autism and developmental disorders, 44, 2981-2995.
Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., … & Halladay, A. (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. Journal of autism and developmental disorders, 45(8), 2411-2428.
Scully, M., Couger, K., & MacDonald, R. (2023). Assessment and treatment of stereotypy in infants at risk of autism spectrum disorder. Behavioral Interventions.
Sheinkopf, S. J., Iverson, J. M., Rinaldi, M. L., & Lester, B. M. (2012). Atypical cry acoustics in 6‐month‐old infants at risk for autism spectrum disorder. Autism Research, 5(5), 331-339.z
Sheldrick, R. C., Schlichting, L. E., Berger, B., Clyne, A., Ni, P., Perrin, E. C., & Vivier, P. M. (2019). Establishing new norms for developmental milestones. Pediatrics, 144(6).
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2016). Vineland Adaptive Behavior Scales (3rd ed.). Circle Pines, MN: American Guidance Service.
Stallworthy, I. C., Lasch, C., Berry, D., Wolff, J. J., Pruett Jr, J. R., Marrus, N., … & IBIS Network. (2022). Variability in responding to joint attention cues in the first year is associated with autism outcome. Journal of the American Academy of Child & Adolescent Psychiatry, 61(3), 413-422.
Squires, J., Bricker, D. D., & Twombly, E. (2009). Ages & stages questionnaires (pp. 257-182). Baltimore: Paul H. Brookes.
Vismara, L. A., & Rogers, S. J. (2010). Behavioral treatments in autism spectrum disorder: what do we know?. Annual review of clinical psychology, 6, 447-468.
Zwaigenbaum, L., Brian, J., Smith, I. M., Sacrey, L. A. R., Franchini, M., Bryson, S. E., … & Roncadin, C. (2021). Symptom trajectories in the first 18 months and autism risk in a prospective high‐risk cohort. Journal of Child Psychology and Psychiatry, 62(12), 1435-1443.
Authors
MacDonald, Rebecca P. F., PhD
The New England Center for Children, Southborough, MA, USA
Department of Psychology, Western New England University, Springfield, MA, USA
https://orcid.org/0000-0003-3614-2134
Couger, Kathryn, MA, MS
The New England Center for Children, Southborough, MA, USA
Department of Psychology, Western New England University, Springfield, MA, USA
https://orcid.org/0000-0001-7470-800X
Yarzebski, Victoria, MSEd, MS
The New England Center for Children, Southborough, MA, USA
Department of Psychology, Western New England University, Springfield, MA, USA
https://orcid.org/0009-0001-3136-5083





