
Introduction
This project is being carried out in Uruguay, a little country located in the south of South America, between Argentina and Brazil. Uruguay has a population of 3.300.000 inhabitants and half of them live in the Capital City (Montevideo).
At present, substantial changes in the Public Health Policy are being introduced in our country. There is high interest in the implementation of programs for the promotion of health and education about health at the primary level of care. Theseprograms, many of which are already in progress, are especially aimed at infants and their families. Tools and training to detect early indicators of deviations from healthy development are very useful for the purpose of these programs.
Our project offers the possibility of early detection of risk indicators in healthy emotional development during the first years of life. We are part of an international network of teams working with the Alarm Distress Baby Scale ( AlarmeDétresseBébé, ADBB ) under the supervision of Prof. A. Guedeney, Paris, France. One of the main goalsof this projectis to intensify the application of an interdisciplinary approach (pediatricians, day care center staff and infant mental health professionals).We wishto promote a more integrated perspective of the infant’s health by expanding the knowledge that pediatricians have about healthy development in the first years of life. In this way these professionals can become agents of health preventionand early detection.
All the children in our country attend monthly pediatric consultations during the first years of life. This makes the pediatrician the professional with the closest contact with the baby and his/her parents, and, as a result, he is an important reference for the parents. This project considers this regular pediatric consultation as a first approach to infant mental health.
With this in mind, we offer pediatricians a trainingwith the ADBB scale which has been validated by several teams in different countriesand is easy to apply after a brief process of training. This instrument, which we hope is user-friendly, consists of a systematized observation of the baby that has been elaborated for the early detection of risk indicators in emotional development (A. Guedeney, 2001).
In case indicators of risk are detected, and once any possible organic cause for this situation is discarded, this project intends to provide the pediatricians trained in the use of the scale with resources that will enable them to carry out an intervention. These interventions, oriented by the results obtained in the application of the scale, will be implemented in the course of the following regular pediatric consultations and they will be aimed at improving the general condition of the baby. This will be developed further on in the text.The scale will be applied again to these babies, five months after the first application, in order to reassess their condition. This will give us a hint as to how effective the intervention was.Those babies who display signs of severe sustained withdrawal will be referred for further more specific evaluation in view of the high risk this may imply for their healthy development. The general aim of the project is to promote an interdisciplinary model of early intervention for infants at the primary level of care.
Objectives
General objective
Early detection of risk indicators in early emotional development in babies aged between 2 and 24 months, during the pediatric consultation.
Specific objectives
- Early detection by the interdisciplinary teamof withdrawal signals in infants aged between 2 and 24 months using the ADBB scale. (Alarme Détresse Bébé. Guedeney, 2001)
- Training pediatricians in ADBB scale and the provision to them of the necessary resources to implement an intervention with the babies who showed withdrawal signs. These interventions will be oriented by the result obtained in the scale.
- Evaluation, of the degree of reversibility of the withdrawal signs as a likely result of the intervention throughthe pediatricians.
- Expansion of the application of an interdisciplinary approach and promote a more integrated perspective of the infant’s health, making pediatricians aware of the infant emotional life and expanding their knowledge about healthy development in the first years of life.
Background
Over the last few decades, the study of the emotional development during the first years of life has become more and more relevant. Different investigations about several aspects of early infancy have agreed in considering this period as especially sensitive and essential for the development of the human being (Bowlby 1969, Brazelton 1975, Stern 1985, Guedeney 1997, Fonagy 2002).
These studies that came from different disciplines, have allowed health professionals to improve their knowledge about factors and conditions that promote or hinder a healthy development. It has been a challenge for health professionals to put these new scientific advances into practice in the creation of useful instruments for their application in the early detection of health problems during the first infancy.
Video-recorded observations of interactions between mother and baby (Brazelton, 1975) and “still-face” experiences (Tronik, 1978) among others, have shown a baby who has capacities from the very beginning, can show initiative in the interaction with the environment, and has a special sensitivity in the relationship with the other, but at the same time has a very limited range of resources to react to interaction disturbances: protest and withdrawal.
Withdrawal has been considered a natural defense mechanism used by the baby since his first moments of life, in order to regulate the interaction (Brazelton, 1975). But, in certain situations, this resource becomes permanent in the infant’s interactional pattern and inhibits the infant’s capacity to be engaged in an interaction with his environment. This situation could hinder the infant’s physical, cognitive, affective and social development, because the unfolding of his potentialities – in Winnicott´s words – requires, among other conditions, his own active participation (Winnicott, 1960).
Withdrawal in the infant is a sign that points to a disturbance in the dyadic relationship that the baby isn’t able to solve properly (Guedeney, 2004). This disturbance could have different causes that will have to be investigated, and may have its origin in organic or relational difficulties to be found either in the parents or in the baby, or in a failure in the synchronization between them.
This research project assumes that withdrawal, as a clinical phenomenon, is a first symptom of pathology in infancy: depression, developmental delay, attachment disturbances, anxiety, post-traumatic syndrome, sensorial difficulties, abuse, etc (Guedeney, 2007), as well as a sign of a potentially dangerous medical condition. This constitutes an important indication of risk for infant development. The progressive nature of its installation in the baby’s relational pattern makes its early expression hard to detect and easily overlooked in the clinical observation without the help of a specific instrument to detect it.All this justifies the use of the ADBB scale (Alarme Détresse Bébé, A. Guedeney, Paris, 2001) which offers an organized and systematized look at the baby, in order to detect early signs of withdrawal which may be the first indicators of a possible future pathology.
Methodology
Participants
ADBB scale was administered to 73 babies from two populations between the ages of 2 and 24 months according to the range of age in which the scale was validated (Guedeney &Fairmann, 2001).Half of these babies attended their pediatric consultation with one of the pediatricians of our team in a Primary Level Medical Health Center of the metropolitan area of Montevideo, which is dependent on the Public Health Ministry. During four months all the babies within this range of age who attended consultation were evaluated.
The other half was integrated by all the babies between the ages of 2 and 24 months who attended the Day Care Center of the main Public Pediatric Hospital in Montevideo. In the latter case we offered the parents an evaluation through a pediatric consultation that was performed by another pediatrician of our team.
In both populations only healthy babies were included in the project in order to reduce the number of variables to be considered in this sample.Premature and sick babies were excluded. Both populations of infants belonged to families in the average or below average social – economic layer of our society. An important difference between the two populations was that in the case of the Day Care Center, all the babies spend six or more hours a day in the center. Meanwhile, only 9% of the babies from the Medical Health Center attend a one–hour weekly workshop in a Community Center with their mothers. We had no control group, and this is a main limitation of this pilot.
Instrument
ADBB scale is a simple instrument, as far as time and resources are concerned, making the scale accessible for different health professionals after a brief training process and easy to apply in an ordinary situation such as the pediatric consultation with the parent and baby together. It constitutes a guide for the observation of the baby, integrated by 8 specific items, to be observed by the pediatrician during the pediatric consultation( facial expression, eye contact, general level of activity, self – stimulating gestures, vocalizations, briskness of response to stimulation, capacity to engage a relationship, capacity of the child to attract ).Each item can be coded from 0 (no withdrawal signs) to 4 (extreme withdrawal). A total score of 5 or more is considered optimal in detecting infant social withdrawal. (Guedeney &Fairmann, 2001)
This instrument has a good internal coherence ( Cronbach is 0.83 ), and it includes the counter – transferential experience of the professional involved in the evaluation, which provides with a dynamic and clinical profile that enriches the information the tool offers. This characteristic, and its vast possibilities for prevention and education in the field of health during the first infancy, have generated in our team great interest in this instrument.
Since 2001, the ADBB scale has been in the process of validation and use by interdisciplinary teams in different countries, with the purpose of doing research, promoting education about healthy development in infancy with attention to the early developing relationship between babies and parents ( www.adbb.net ). In South America, this experience began in Brazil in 2004 (Lopes, 2004). In the region of the Rio de la Plata in particular, Argentinean professionals, who have a close relationship and regular scientific exchanges with us, have been working for the validation of the scale since 2006 ( Dr. Monica Oliver and Cols. Mental Health Department. German Hospital. Buenos Aires). In Uruguay, the experience with the scale began in 2006, with the work of our interdisciplinary team integrated by a psychoanalyst, two pediatricians and a child psychiatrist.
Procedure
All the babies were assessed duringthe pediatric consultations with the presence of at least one of the parents. Parents who agreed to participate in this experience were properly informed about it and signed an authorization for the eventual use of the tapes in training and scientific events. The video – recorded material was used by our team for the detection of withdrawal signs through the 8 items of ADBB scale.
Infants with withdrawal signs (score more than 4 in the scale), were evaluated again 15 days later, to confirm the score. If thesesigns persisted the pediatrician first tried to detect organic factors that may be causing them (sensorial difficulties, sickness, severe pain, malnutrition). If there were no organic conditions, a relational disturbance was considered the possible cause of the withdrawal signs. If a relational disturbance was the case, we implemented a series of interventions aimed at improving the general condition of the baby. These interventions, oriented by the results obtained in the application of the scale, were carried out by the pediatrician, in the course of the following regular pediatric consultations. The purpose of these interventions is to raise parental awareness of the infant’s health and to promote new resources that can strengthen their capacities to facilitate a healthier relationship with the baby. .Babies with ADBB score > 10, in addition of this intervention, were referred to a more specialized evaluation considering them in a high risk situation for their development.
Interventions
- Point to the capacities that the baby displaysand draw the parents´ attention to the aspects of his/her development that could be improved in view of the results of the scale.
- Promote verbal interchanges with the baby.
- Work with the parents about the baby’s development to help them support the baby’s acquisition of new skills.
- Watchthe video with the parents, drawing their attention to the initiatives of the baby and to the aspects of his/her development that could be further stimulated and impacts the baby’s capacity to interact and enter into a healthier relationship.
- Refer isolated or depressed mothers to a community center in the neighborhood so that they can participate in mother – baby workshops.
After the pediatrician’s interventions during each monthly consultation, and approximately five months after the first application of the scale, the babies were re-assessed by the team with a second application of the ADBB scale in a new video – recorded pediatric consultation.
Institutional intervention: in the case of the day care center, we hold interdisciplinary working sessions with the caregivers to discuss how to promote the development of the babies in view of the scores obtained in the scale.
Results
The experience of three years in the application of the scale has shown similar results found in international investigations carried out in different cultural and social environments (Guedeney-Fermanian 2001; Milne–Greenway–Guedeney-Larroque 2008).
In our research, both populations of babies which were evaluated (Day Care Center and Medical Health Center) showed the same behavioral profile without any significant difference in the square chi (0.068), and therefore the overall study sample included 73 babies (graph 1).
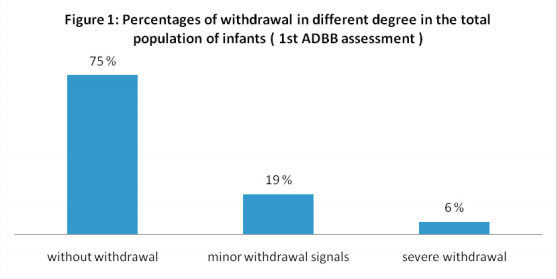
In this population of babies, 25 % presented withdrawal signs in the first assessment. Minor withdrawal signs (scores 5 to 10) were detected in 19% of the babies, and 6% of the babies presented more severe and evident withdrawal signs (scores > 10).
We could follow up 14 of the 18 babies that had presented withdrawal signs, because of changes in their address or in the place that they receive medical assistance. We couldn´t follow up 3 babies with a score from 5 to 10, and 1 with a score > 10.
In the second assessment, we found that all the babies with minor withdrawal signs (scores between 5 and 10) fully improved their condition, except for a baby girl who was undergoing a difficult emotional situation because of the recent divorce of her parents. The effect of the intervention was more varied in the babies that presented more severe and evident withdrawal signs (score > 10). (Graph 1)
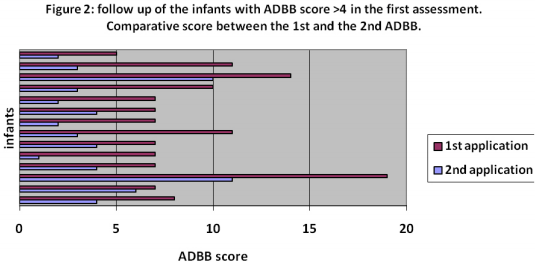
To measure the impact of the process of intervention and follow up, we carried out a comparative analysis of the results obtained by these babies in the first application of the scale and in the second one.In the second assessment five months after the first application, we found that all the babies who had first presented withdrawal signs in different degrees (25% of the entire population) showed total or partial improvement ( graph 2 ).All the babies with minor withdrawal signs (score between 4 and 10) fullyimproved, except for a baby girl who was undergoing a difficult emotional situation because of the recent divorce of her parents. In the case of babies with severe withdrawal ( score > 10 )who were in a referral process to be evaluated and eventually treated by specialists, we observed that the effect of the intervention was more varied. Even when in all these cases there was a certain reversibility of the withdrawal signs, in most of them it wasn´t enough to recover the health state of the baby. A more precise study about this population of babies will be worked by the team with a larger population.
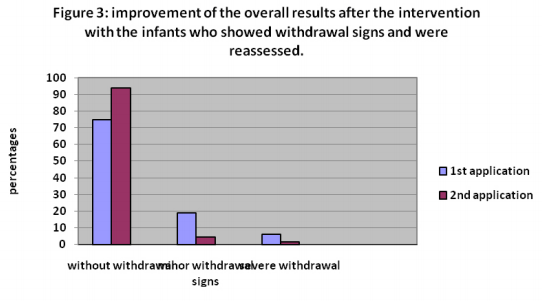
If we consider the scores obtained in the second application of the scale, we observe, that the percentage of babies without withdrawal signs increased from 75% to 94%, and the percentage of babies with withdrawal signs in different degrees decreased from 25% to only 6% ( with 4.5% of the babies with minor withdrawal signs and 1.5% with major ones)(graph 3).
Discussion
This study has several limitations. Firstly it is necessary to work in the future with a methodological design that include a control group to try to measure in a more precise way the impact of the intervention in the condition of the baby.We also need to work with a larger population of babies that allows us the assessment and follow up to a higher number of babies with sustained withdrawal signs. We are starting a new study with this purpose.
In our population thepercentage of babies with withdrawal signs is higher than the one detected in the studies carried out in France (11 %), Israel (11,6%) and Finland (4 %), but it is lower than the results obtained in Australia (27%). It is possible to consider that the high percentage of babies with withdrawal signs found in the population we evaluated might be influenced by the socio – economic situation of their families, which could be identified as a population at risk. This hypothesis must be confirmed by further research.
This experience has provided us a first perception which suggests that the majority of the infants with withdrawal signs could present a reversible condition and they could recover their developmental capacities before this situation becomes pathological. At a preliminary glance, this improvement seems to be the result of the intervention and follow up by the pediatrician integrated in a team with mental health professionals, in the primary level of care.
Based on this experience, we observed that once the difficulties detected in the baby are pointed of to his caregivers, it becomes the beginning of an intervention that engender their recognition of new resources that will help at improving the baby’s condition.In the future we may offer pediatricians training aimed at deepening their knowledge in the specific items of the scale and being more focused in their intervention to the unique characteristics of each infant and parent.
Conclusions
Through this experience, we have observed that the application of the scale in the pediatric consultation allows for a more global and systematized perspective of infant development and relational capacities. In the context of the services provided to the community of babies and parents in Uruguay, this is a start for increasing the awareness among pediatricians and parents of the infant’s needs and development, and of the potential for change.In the light of these preliminary results, we aim in the future to look more precisely at the content of the intervention, especially for those infants with high scores of sustained withdrawal signs.
Keywords: Infancy, interdisciplinary studies, early detection, sustained withdrawal, early emotional development
Acknowledgments
The International Psychoanalytic Association and the Latin American Psychoanalytical Federation elected this Project for the 15th Research Training Program which was held in the University College of London in August 2009, and this participation was supported financially by both institutions. Dr. P. Fonagy and Dr. R. Emde were the mentors of this project. We thanks to their contributions and the ones from the fellows of the program to continue with a new step of our study.
References
Brazelton, 1975. Early mother-infant reciprocity in parent-infant interaction. Infant Behavior and Development. Elsevier Scientific Publishing.
Bowlby, 1969. Attachment and Loss. Nueva York. Basic Books.
Bowlby, 1982. Attachment and Lost: retrospect and prospect. American Journal of Orthopsychiatry, Vol.52 No 4, 664-678.
Dolberg, Keren et al. 2006. Sustained withdrawal behavior in clinic – referred and nonreferref infants. Infant Mental Health Journal, 27 (3), 292 -309.
Fonagy, 2002. Affect regulation, mentalization and the development of the self. New York. Other Press.
Guedeney, 1997. From early withdrawal reaction to infant depression: a baby alone does exist. Infant Mental Health Journal, 18(4):339-49.
Guedeney, Fermanian, 2001. A validity and reliability study of assessment and screening for sustained withdrawal reaction in infancy : the Alarm Baby Distress Scale. Infant Mental Health Journal, 22:559-575
Guedeney, 2004. Comportement de retrait relationnel de jeune enfant. Médicine Sciences, Vol.20, No. 11.
Guedeney, Foucault, Bougen, Larroque, Mentré, 2007. Screening for risk factors of relational wihdrawal behavior in infants aged 14-18 months. European Psychiatry, 1-6.
Lopes, Ricas, CotaMansini, 2004. Alarm Distress Baby Scale. Evaluations of the psychometrics among 122 Brazilian Children. org.congress2004
Milne, Greenway, Guedeney, Larroque, 2009. Long term developmental impact of social withdrawal in infants. Infant Behavior and Development.
Mirjami, Kaija, Luoma, Pälvi, Raili, Tuula, 2008. Infant´s social withdrawal and parent´s mental health. Infant Behavior and Development. Elsevier Scientific Publishing.
Stern, 1985. The interpersonal world of the infant. Nueva York. Basic Books.
Tizón, Izquierdo, Nadal, 2002. Traducción y retraducción al castellano de la escala ADBB. Unitat de Salut Mental de Sant Martí Nord.
Tronik, 1978. The infant response to entrapment between contradictory messages in face-to-face interaction. Journal of American Academy of Child Psychiatry. Vol. 17.
Bonifacino, Musetti, Hackenbruk, Schelotto, Fostell, Pereira. Estudio de señales de retraimientodelbebé. Rev. de la Asociación de Psiquiatría y Psicopatología de la infancia y la Adolescencia, APPIA. N 16. Uruguay.
Bonifacino, Musetti, Hackenbruk, Schelotto, Fostell, 2007. Estudio de señales de retraimientodelbebé clinique transculturelle. Site: adbb.net
Winnicott, D. 1960. The theory of parent – infant relationship. in The maturational processes and the facilitating enviorment. Ed. Laia. 1981. Barcelona.
Affiliates Corner: The Pediatric consultation: A first encounter with infant mental health
Authors
Nahir Bonifacino (Psychologist, Psychoanalyst)
Dora Musetti (Child Psychiatrist),
Andrea Plevak and Magdalena Schelotto (Pediatricians),
Uruguay





