
Introduction
Infant and Early Childhood Mental Health Consultation (IECMHC) is a capacity-building, prevention-based, multi-level service where mental health professionals collaborate with child-serving staff and families to promote healthy social-emotional development among young children (Tidus et al., 2022). The evidence base for IECMHC has grown substantially over the past several decades, with numerous studies demonstrating its effectiveness in improving child outcomes, enhancing teacher practices, and reducing early childhood expulsions (Center of Excellence, 2021; Tidus et al., 2022). Despite these positive findings, significant racial disparities persist in early childhood settings (Iruka, Curenton, & Durden, 2017). Young Black boys and children with disabilities continue to experience disproportionately high rates of expulsion and suspension (U.S. Department of Education, 2024).
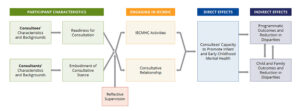
Recently, the Center of Excellence for IECMHC, funded by the U.S. Substance Abuse and Mental Health Services Administration, disseminated a theory of change that articulates how IECMHC works to impact directors, teachers, children, and families (See Figure 1, below; Center of Excellence, 2021). A recent literature synthesis on IECMHC highlights the strengths and gaps within the extant literature on IECMHC and directions for future research, including examining different experiences and impacts, strengthening study design and measures, and “expanding the methods used to acknowledge non-Western ways of knowing and to honor community voice and personal narrative as valid sources of data.” (Tidus et al, 2022, p.18). These recommendations, along with best practice guidance, are helpful, yet there is a need for practical guidance on how to operationalize them in evaluations of IECMHC.
Traditional IECMHC evaluation approaches have often overlooked examining how consultation services are experienced across different racial and ethnic groups and have typically neglected to consider how the racial and cultural identities of consultants might influence their work with diverse populations. To decolonize IECMH and consultation, it is necessary to create spaces to identify how racism has and is operating in both practice and research, and also address it, while also promoting collaborative relationships and collective healing through research to improve practice, professional development, and research. To facilitate this process, it is important to acknowledge the paradigms guiding who we are, how we are, and what we do as researchers and evaluation partners in this work. Datta (2018) highlights that being oriented and trained within western or eurocentric paradigms leads to more positivist worldviews and subsequent practices such as seeking a single truth rather acknowledging the existence of multiple truths, privileging objective scientific discovery over subjective and experiential knowledge, and promoting objectivity and detachment rather than partnership and collaboration. Our capacity to decolonize IECMH and consultation is built on the extent to which we can acknowledge and take intentional action to unlearn, learn, and adopt more African-centered, indigenous, and other nondominant paradigms. Doing so will facilitate a more transformative and empowering experience for the researchers and participants (Datta, 2018). This paper describes our team’s efforts to develop and implement a decolonized, racial equity-centered approach to evaluating an established IECMHC program within a northeastern metropolitan community.
Program Context and Evaluation Framework
The IECMHC program that participated in this project provides embedded consultation services to child development centers (CDCs) in a metropolitan region of the U.S., primarily serving Black and Latine populations in historically underserved communities. The program has been in existence for over a decade and has recently undergone significant expansion, tripling its consultant workforce and the number of CDCs it serves.
Our evaluation framework was co-created through a partnership between a university-based team of academic researchers, several with clinical experience, and the local government agency that operated the IECMHC program. Our team’s lived experiences, training, and anchoring in the Center of Excellence for IECMHC Theory of Change (ToC; Center of Excellence, 2021) provided a foundation on which to intentionally center equity in our evaluation. We deliberately expanded the ToC framework to incorporate explicit considerations of racial equity—a response to the IECMHC field’s recent revision of professional competencies to elevate equity concerns in service delivery and evaluation (Schoch et al., 2024). We also used the Equitable Evaluation Framework, which offers guidance in how to center equity in evaluation by exploring, questioning, learning, and unlearning in ways that help inform actions and decisions (Equitable Evaluation Institute, 2025). This framework assisted our team in operationalizing equity and applying the ToC in our evaluation.
Community-Engaged Evaluation Methods
Centering racial equity in our evaluation approach began with the composition of our team. The five-member evaluation team included researchers with diverse racial and ethnic backgrounds: three members identify as white, one as Black/African American, and one as Hispanic/Latina. With varied backgrounds, education in public health, psychology, and social work, as well as professional development and work experiences, this diversity brought varied perspectives to our evaluation design, interpretation of findings, and dissemination. See the team’s positionality statements in Figure 2. Despite this diversity in backgrounds and lived experience, each of the team had formal training in positivistic research paradigms which informed our approach. And the funder and local decision makers sought empirical data to answer the question: was fidelity maintained when the expansion was implemented?

Note. This visual depicts our team’s positionality statements, which highlight our team’s racial and cultural identities, backgrounds, and lived experiences, and how they intersect with our evaluation and research work in infant mental health.
Community Engaged Approach
We employed community-engaged methods to align our evaluation priorities with the concerns and interests of those most affected by the program. There were multiple time points at which our team encountered equity-focused decision-making. These are depicted in Figure 3. Prior to finalizing our evaluation protocol, we conducted “community listening sessions” with consultants and supervisors to understand which program components warranted the closest examination through a racial equity lens, and what they desired to learn through the evaluation. These sessions revealed concerns about the consistent implementation of the model across diverse populations and curiosities about cultural responsiveness in service delivery and evaluation. We listened and heard the unique experiences of staff given various racial and cultural backgrounds, educational experiences, time working in the program, and communication style differences. Therefore, we decided that it would be helpful to offer the opportunity to share experiences with us through surveys, interviews, and focus groups. Given the sensitivity in talking about race and racialized experiences, we solicited the participants’ preferences for racial affinity in interviews and focus groups.
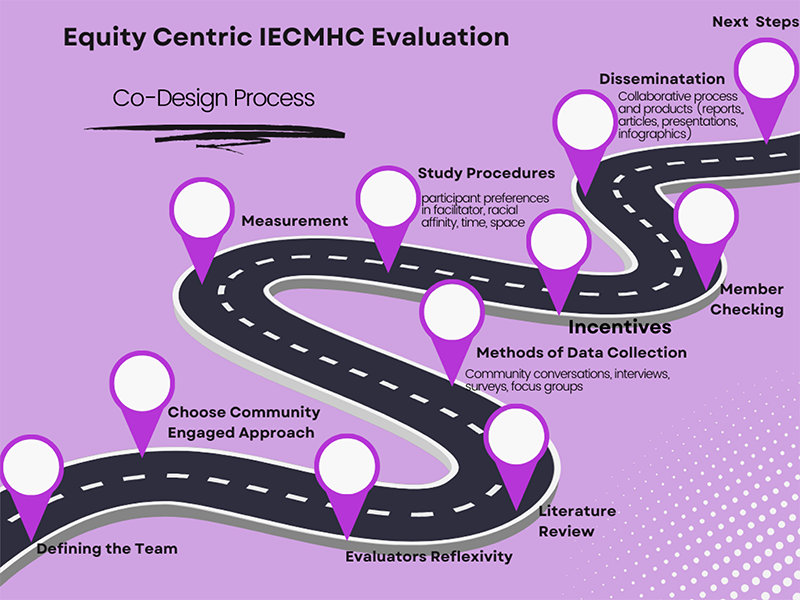
Note. This visual demonstrates some of the steps in our equity-centered decision-making process to ensure that equity remains a priority in our evaluation.
Researcher Reflexivity
Research reflexivity was essential in our team’s approach and a way to reflect before, during, and after engaging with our community partners. Some of the questions offered for individual reflection after interviews or focus groups and team debriefing process included:
- What is staying with you? What did you learn? Did anything surprise you?
- What evoked emotion within you during the experience? What happened and what emotions were present?
- Given your social location or experiences, how did the question on racialized experiences go?
- Is there anything else that you think would be helpful to consider as we continue?
A couple of the themes that emerged from our reflections and debriefing included increasing awareness of how social location and racialized issues emerged–and maybe more importantly–failed to emerge in the context of the IECMHC program and the evaluation, and how the individual team members could reflect on their own positionality in relation to the conversations that were had with consultants and supervisors. We had to navigate our emotions and determine how to respond to sensitive matters or the unexpected shared with the evaluation team. A reflection shared by AP:
“I remember feeling really happy, like really happy when I heard that consultants that were Black were working with predominantly Black programs and most had Black supervisors. I know it sounds biased, but as a Black woman and past consultant who never had a Black supervisor–and wanted one, this really stayed with me. No code switching with families, directors, or in supervision–that sounds amazing, way less exhausting. Another strong emotion that stayed with me was about how a racial incident shared with me was handled. Racial issues happen every day but I felt this in my body, it did not sit well with me. As I struggled to manage my emotions, I also felt I had to be really careful about what I said given the situation, yet also show up authentically and respond sensitively. That was hard.”
Another team member [SM] wrote these reflections:
“I was really struck by her comment that teachers feel bias from kids, because in my head they’re less-biased. But I know that was too quick an assumption for me to make – my own kids started verbalizing racial generalizations around age 4.”
Throughout the evaluation process, we maintained a reflective and collaborative approach within our team and with the mental health consultation program partners. We prioritized sharing preliminary findings and soliciting feedback on data interpretation. This approach builds on and embodies Shivers and colleagues’ (2022) work and can be described as “de-colonizing” evaluation practices by shifting power dynamics and privileging the interpretations of those closest to the work.
Measurement and Data Collection Approaches
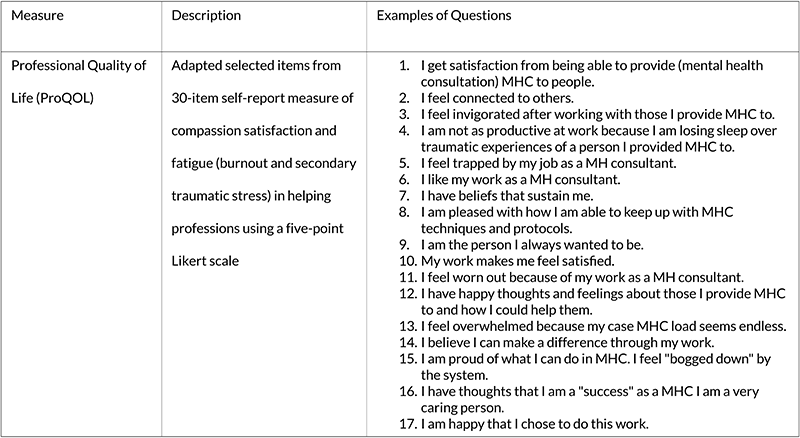
Our evaluation employed a mixed methods measurement approach that captured multiple dimensions of IECMHC implementation through a racial equity lens (Table 1). By examining consultants’ racialized experiences, ensuring linguistic accessibility, and gathering data from multiple perspectives, we strove to identify strengths and disparities in program understanding, engagement, and satisfaction across different racial, ethnic, and linguistic groups.
Table 1. Key Measures Used in the IECMHC Evaluation.
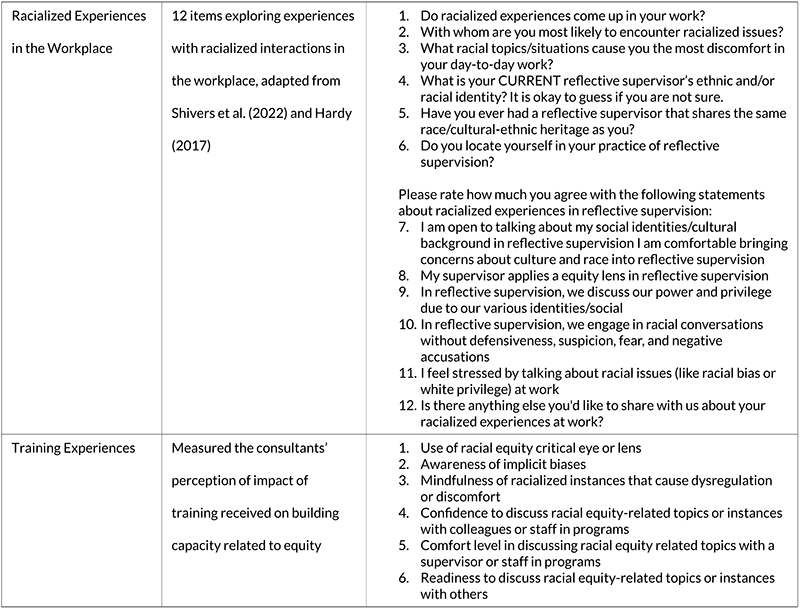
Consultant Well-being and Experiences: We conducted individual interviews and focus groups with consultants. The interview and focus group guides included questions about their thoughts about the program, their hopes in the evaluation, and their experiences as consultants, and in particular training and reflective supervision experiences, racialized experiences, management of stress, and supports for their mental health, and wellness. Given the nature of the dialogue, we asked the consultants about their preferences to be interviewed by different members of our racially and linguistically diverse team. This allowed our team to facilitate racial matching in the interviewing process, if desired and acceptable. We used rapid qualitative analytic methods to analyze the interview data, which proved helpful in quickly translating the findings for member checking to ensure adequate representation and use of the findings to inform continuous quality improvement within the IECMHC program.
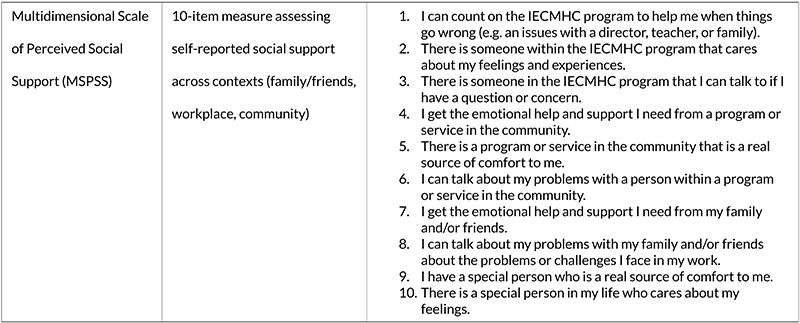
We measured consultants’ professional quality of life using the Professional Quality of Life. Professional Quality of Life (ProQOL) (Hudnall Stamm, 2009), which assesses compassion satisfaction, burnout, and secondary traumatic stress. We recognized that consultants’ ability to effectively serve diverse communities might be influenced by their own well-being and support systems, so we also measured perceived social support using an adapted version of the Multidimensional Scale of Perceived Social Support (MSPSS) (Zimet et al., 1988). Our adapted version focused on the perception of support across contexts, specifically support from someone close to them (romantic partner), family or friends, work, and community.
Of particular importance to our racial equity focus, we included measures of racialized experiences in the workplace, adapted from prior work by Shivers et al. (2022). These items examined encounters with racial issues, comfort discussing race and culture in reflective supervision, and experiences of racial microaggressions. Additionally, items were developed to identify consultants’ self and community care practices.
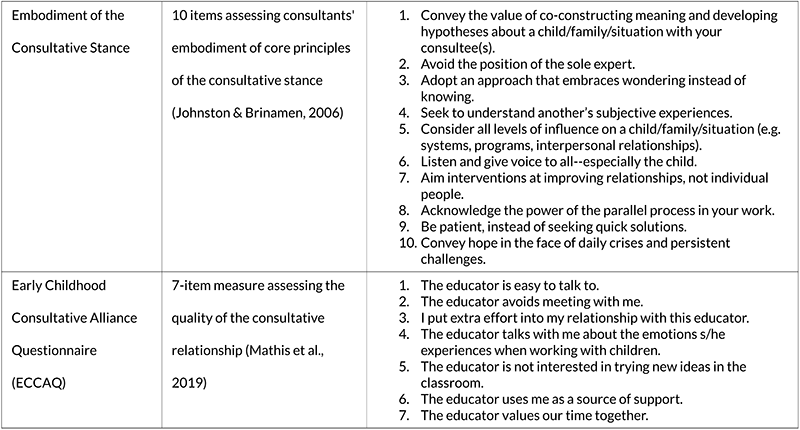
Consultative Approach and Relationships: We developed a novel measure to assess consultants’ embodiment of the consultative stance based on Johnston and Brinamen’s (2006) framework. This measure captured consultants’ approach to their work through 10 items corresponding to core tenets such as “avoid the position of sole expert” and “seek to understand another’s subjective experiences.” The consultants’ understanding and intentions on mitigating the power imbalances and capacity for empathy are important areas of development in decolonizing infant mental health work (Mullan, 2023). Both consultants and supervisors completed this measure, allowing for multi-perspective assessment. The quality of consultative relationships was measured using a selected (or a subset of) items from the Early Childhood Consultative Alliance Questionnaire (ECCAQ) (Mathis et al., 2019), with consultants rating their relationships with selected teachers and teachers rating their relationships with consultants. An innovation in this approach was asking the consultants to rate teachers that they were working with and felt they had both a positive and negative consultee relationships with.
Reflective Supervision: Recognizing the importance of reflective supervision in supporting consultants’ work, we assessed both consultants’ experiences of supervision (using the Reflective Supervision Rating Scale RSRS; Gallen et al., 2016) and supervisors’ confidence in providing effective reflective supervision (using the Reflective Supervision Self-Efficacy Scale for Supervisees RSSESS; Shea et al., 2020). These measures allowed us to examine the extent to which reflective supervision supported consultants in general, and specifically in creating a safe enough space to increase reflective capacity and action for equity.
Various Community Partner Perspectives: We gathered data from multiple community partner groups (CDC directors, teachers, and families) to examine how IECMHC was experienced across different groups. The Family Experiences Survey, developed specifically for this evaluation, included questions about program understanding, comfort discussing mental health, and service satisfaction. Importantly, this survey was available in both English and Spanish to ensure linguistic accessibility. Teacher and Director Surveys assessed perceptions of service helpfulness, knowledge gains, and practice changes resulting from consultation. Incentives were offered to community partners to compensate them for their time and contributions. Creating space to be informed and guided by families and early childhood program staff enhances the program’s services and evaluation in a number of ways, including helping to shift and share power.
Implementation Fidelity: We developed a comprehensive set of fidelity metrics based on the Center of Excellence for IECMHC’s essential elements framework (Schoch et al., 2024) and the Healthy Futures program model. These metrics were calculated using administrative data from their data management system and covered three levels of consultation: programmatic (CDC-level), classroom, and child-specific. This approach allowed us to pinpoint places where the quality of the implementation fidelity was not high enough to address disparities as intended, which identified critical areas for program quality improvement.
Analysis
The analysis and write-up of the findings presented another step in our evaluative process, and like other steps, it too presented both opportunities and challenges as we tried to center equity in our evaluation. Despite our best efforts to balance the use of qualitative methods with validated tools, we found ourselves limited in what we could say about any of the important constructs we sought to elevate. The small sample size for this evaluation (n=17 consultants; n=65 teachers; n=20 directors of CCDs; and n=73 families served) reduced our ability to say anything conclusive about the quantitative data from the surveys. The intimate nature of the programmatic team made it difficult for us to protect the anonymity and confidentiality of the respondents in the qualitative analysis. In the end, the underlying tension that emerged from our own internal struggles against our positivist training left some on the team feeling frustrated by the “findings” as we summarized them for the program partners. Some on our team, in particular our white researchers, had worked hard to use all the “best” tools and measures to try to quantify what we believed to be important empirical components of the program’s implementation; concurrently, “our Black researcher [AP] was leaning in to the relational, qualitative work that shed insight into the consultants’ experience implementing this complex intervention in a dynamic and racially charged context. In the end, as a team, we questioned the extent to which this approach allowed us to do either one as well as we would have liked.
Dissemination
What we did do well was to stay true to our collaborative, reflective, and intentional evaluation framework from the start to the end of this project. We prioritized dissemination activities and deliverables that were most helpful to the IECMHC program; therefore, we shared findings back through a newsletter, a presentation that was delivered to staff live and recorded via Zoom, and a written report. Of no surprise, at the culmination of this work, it was clear that our relationships and this work had just begun, as in the conversations with the program leadership and consultants the sense of safety that grew overtime, and at the end, there was more comfort in dialogue and explicit sharing with our team, and in particular AP about racialized experiences and goals to advance equity. This was a really meaningful outcome. We also shared this work in a national conference alongside other IECMH researchers and invited the IECMHC program to provide feedback on our presentation, and participate in the session, if desired. While the project ended, at the close of the funded work, our evaluation team and the IECMHC program remains in community, and intends to continue the mutually beneficial relationship in the continued dissemination of this work, and also in partnership in the advancing equity and IECMHC through policy, practice, and research.
Conclusions
Our evaluation of the IECMHC program demonstrates both the importance and feasibility of centering racial equity and using decolonizing practices within IECMHC program evaluation. Through this work, we captured a snapshot of the experiences of consultants and their supervisors, as well as the teachers, directors, and families served. The co-constructed mixed-methods design with prolonged, collaborative, and deeply reflective engagement created space for the exploration of IECMHC within the context of racialized experiences, equity, as well as the promotion of wellness and healing among consultants and those they serve.
Decolonizing IECMH starts with us (Mullan, 2023). Research is a powerful force—guiding thought, feelings, and actions (or inaction) in our field. This work represents a paradigm shift; we are not separate, we are creating spaces through research that can be decolonizing by asking about history, experiences of racism, and healing. We have the opportunity to shift the narrative about research and researchers. The act of engaging in research and dissemination such as this, using decolonized practices, challenges our training as researchers, and can be a form of resistance and even liberating for both researchers and participants (Datta, 2018). When we include those with lived experiences meaningfully, allow them to lead the work, and provide training and reflective spaces for professional development and healing in the context of our research and evaluation work: This type of research is resistance.
Acknowledgements
We are deeply grateful for the contributions of the infant and early childhood mental health (IECMH) consultants, supervisors, program leaders, directors, teachers, and families who partnered with us and/or participated in this collective work to advance equity in IECMH. Thank you for sharing your truth with us and allowing us to be a part of the journey and storytelling.
Author Note
This research was approved by the Georgetown Institutional Review Board: Study 00006711. The authors have no conflicts of interest to report.
Any correspondence about this paper should be sent to Amittia Parker at Thrive Center for Children, Families, and Communities, Georgetown University, 2115 Wisconsin Avenue NW, 6th Floor Washington, DC 20007. Email: Amittia.parker@georgetown.edu
References
Center of Excellence for Infant and Early Childhood Mental Health Consultation. (2021). Theory of Change for Infant and Early Childhood Mental Health Consultation.
Datta, R. (2018). Decolonizing methodologies: A transformation from science-oriented researcher to relational/participant-oriented researcher. American Indian Culture and Research Journal, 42(1), 115-130.
Equitable Evaluation Institute. (n.d.). Framework. Equitable Evaluation Framework. https://www.equitableeval.org/framework
Gallen, R. T., Ash, J., Smith, C., Franco, A., & Willford, J. A. (2016). How do I know that my supervision is reflective? Zero to Three, 37(2).
Hudnall Stamm, B. (2009). Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL).
Iruka, I. U., Curenton, S. M., & Durden, T. R. (Eds.). (2017). African American children in early childhood education: Making the case for policy investments in families, schools, and communities. Emerald Group Publishing.
Johnston, K., & Brinamen, C. (2006). Mental Health Consultation in Child Care: Transforming Relationships among Directors, Staff, and Families. Zero to Three.
Mathis, Davis, Hunter, & Hartz. (2019). Early Childhood Consultative Alliance Questionnaire Consultant Version (ECCAQ-C). Unpublished instrument. Georgetown University, Washington, DC.
Mullan, J. (2023). Decolonizing therapy: Oppression, historical trauma, and politicizing your practice. WW Norton & Company.
Schoch, A. D., Tidus, K. M., Catherine, E., Perry, D. F., Duran, F., & Rabinovitz, L. (2024). Essential elements of infant and early childhood mental health consultation: Inside the black box of preschool expulsion prevention. Early Childhood Research Quarterly, 66, 24-33.
Shea, S. E., Jester, J. M., Huth‐Bocks, A. C., Weatherston, D. J., Muzik, M., Rosenblum, K. L., … (2020). Infant mental health home visiting therapists’ reflective supervision self‐efficacy in community practice settings. Infant Mental Health Journal, 41(2), 191-205.
Shivers, E. M., Janssen, J. A., Subramaniam, A., Parker, A. L., Noroña, C. R., Lara, C., Best, D., Yazzie, D. A., Cimino, J., Kohchi, J., Fitzgibbons, S. (2022). Digging Deeper: De-Colonizing Our Understanding and Practice of Reflective Supervision Through a Racial Equity Lens. https://bit.ly/46QIS5E
Tidus, K., Schoch, A. E. D., Perry, D., Rabinovitz, L., & Horen, N. (2022). The evidence base for how and why infant and early childhood mental health consultations works. HS Dialog: The Research to Practice Journal for the Early Childhood Field, 25(2).
Toliver, S. R. (2021). Recovering Black storytelling in qualitative research: Endarkened storywork. Routledge.
U.S. Department of Education, Office of Civil Rights. (2024). http://www.ed.gov/ocr.
Zimet, G.D., Dahlem, N.W., Zimet, S.G., Farley, G.K. (1988). The Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment, 52, 30-41.
Authors
Parker, Amittia
Georgetown University,
Washington, DC, USA
Castellanos González, Natalia
Georgetown University
Washington, DC, USA
Mitchell, Stephanie
Georgetown University
Washington, DC, USA
Hartz, Karyn A.
University of Rochester
Rochester, NY, USA
Perry, Deborah F.
Georgetown University
Washington, DC, USA





