
Declarations
Funding Statement: This research was funded through a grant from the DC Department of Health (CHA2020-000004).
Conflicts of Interest: Aza Nedhari serves as the Executive Director of Mamatoto Village and is the organization’s co-founder. Erin Snowden is the Director of Data and Social Impact and Rabiyah Amina was the Research Specialist at Mamatoto Village. Deborah Perry was paid as an independent consultant to Mamatoto Village to complete the development of this manuscript after a sub-award to Georgetown University concluded.
Ethics Approval: Ethical approval for this study was obtained by the Georgetown University Institutional Review Board (STUDY00002183).
Consent to Participate: Clients in the qualitative study cited in this paper provided informed consent in accordance with the IRB protocol listed above.
Availability of data and material: Data from this study are not available to the public given the small sample size would compromise the confidentiality and anonymity of the clients.
Authors’ Contributions: The authors confirm their contribution to the paper as follows: program conception and design: A. Nedhari; data collection: E. Snowden, R. Amina; draft manuscript preparation: E. Snowden, A. Nedhari, D. F. Perry, R. Amina. All authors reviewed the results and approved the final version of the manuscript.
Authors’ Permission Statement: The authors E. Snowden, A. Nedhari, D. F. Perry, and R. Amina grant WAIMH permission to publish the included photographs in Perspectives and on all WAIMH printed and online platforms.
Photography Credit: Photograph credit for all included photographic images belong to D2D Focus (2025).
Background
Across the United States, Black women are impacted by a persistent maternal health crisis, experiencing a maternal mortality rate 2.6 times higher than that of White women (Hoyert, 2023). Despite being the capital of one of the wealthiest nations in the world, Washington, DC, is emblematic of this national emergency. In 2018, the DC City Council responded to this public health emergency by establishing the Maternal Mortality Review Committee (MMRC), a group tasked with identifying the root causes of maternal mortality and advancing promising solutions. By 2020, Aza Nedhari, Executive Director of Mamatoto Village (MV), one of DC’s most respected community-based perinatal support organizations, was appointed co-chair of the committee. Under her leadership, the MMRC’s 2021 report revealed that between 2014 and 2018, the city’s pregnancy-related mortality rate was 44.0 deaths per 100,000 live births, as compared to 28.4 deaths per 100,000 for the United States during that same period (Office of the Medical Examiner, 2021).
Although Black women constitute approximately 50% of all births in DC, they account for 90% of all pregnancy-related deaths and 93% of pregnancy-associated, non-related deaths. In contrast, White women account for none. Although shocking, these disparities are not a new phenomenon, but rather a reflection of deeply rooted structural inequities shaped by centuries of systemic racism, medical abuse, and systemic destabilization and vilification of community-based solutions such as Grand Midwives who long acted as a protective factor against obstetric harm (Menzel, 2021). In the face of these injustices, Black women are reclaiming their position in birth work. As an act of service and protest, Black women are creating the solutions they need to thrive by prioritizing culture and communal care, demanding reproductive justice, and determining exactly how that vision is achieved.
Inspired by their own life experiences, Mamatoto Village co-founders Aza Nedhari and Cassietta Pringle entered the field of birth work by completing a national doula training that they believed fell short in delivering the core competencies, skills, and community relevance necessary for providing meaningful and effective care. They believed Black women deserve dignity, respect, and care reflecting their experiences. Together, they committed to providing services built on cultural congruence, a practice beyond shared racial identity and surface-level awareness. Cultural congruence is a reciprocal process between the client and provider that fosters trust and improves outcomes through a deep commitment to delivering care that is respectful of and responsive to the cultural values, beliefs, and practices of clients and their families. With this understanding, they created Mamatoto Village, a community-led perinatal health organization in Washington, DC, dedicated to equipping Black families with the support, education, and resources needed to experience healthy pregnancies, self-determined parenting, and holistic well-being.
Mamatoto is the Swahili word for mother-baby, reflecting the unique connection in the mother-child dyad. Additionally, the term “Village” emphasizes the importance of a supportive community. This understanding guided the founders’ vision for the organization: “Healthy Mamas, Healthy Babies, Healthy Communities.” This vision is operationalized through an array of innovative programs, training, and services that acknowledge the historical and systemic challenges that have led to persistent perinatal health disparities, while also celebrating the resilience of the families seeking care at MV. Services are offered in a physical space located within the DC neighborhood where most of the program’s clients reside. It is more than a provider’s office, but a warm and welcoming second home filled with vibrant colors, textures, art, and photographs that celebrate the beauty and diversity of Black culture. This space is unapologetically Black, designed to feel familiar and affirming to the clients, staff, and the community it serves.

Program Description
An Evidence-Informed Solution: Mothers Rising Home Visiting
One of the primary vehicles MV uses to deliver quality services to clients is through Mothers Rising Home Visiting (MRHV), a strengths-based perinatal home visiting program that builds social capital for Black women in DC. The program has three main goals: 1) improve perinatal outcomes, 2) prevent and reduce maternal mortality and severe morbidity, and 3) increase family stability. MRHV recognizes that individuals are the sole experts on their lives. Therefore, the care journey begins with a comprehensive biopsychosocial intake assessment that considers not just pregnancy but the complete social and cultural context in which the participant lives. Using the results of the assessment, the MRHV team partners with the participant to co-create an individualized care plan outlining the provision of nonjudgmental, culturally congruent care to reduce the impact of socio-economic burdens, provide care coordination, counseling, and health education, and help build a support system resulting in more positive perinatal and infant health outcomes.
An innovative aspect of MRHV is that it is simultaneously supported by a robust workforce development program. In addition to providing home visiting services to at least 300 clients per year, MV has trained over 200 perinatal health workers (PHW). PHWs are primarily Black women from the MRHV service area – including former program clients – who complete one of MV’s workforce training pathways, particularly the Perinatal Community Health Worker (PCHW), a term and training model coined and developed by Mamatoto Village in 2015. The PCHW training is a 225-hour immersive experience grounded in a human rights, reproductive, and birth justice framework. The curriculum provides foundational knowledge of public and community health, documentation and charting, the history of obstetrics and midwifery in the US, as well as an analysis of systemic and structural racism, and its impact on perinatal health and parenting experiences of Black people. Additionally, it entails an understanding of preconception health, the physiologic changes during the perinatal period, nutrition, the stages of the birthing process, including labor support techniques; newborn care; pregnancy and postpartum complications, loss; perinatal mental health; intimate partner violence and substance use disorder; care coordination and resource navigation; lactation; and reproductive health. Bridging evidence that supports both doula and community health worker (CHW) models, this training program goes beyond these traditional pathways and is a 1) pathway for Black women into sustainable careers that drive community transformation and diversify the perinatal workforce to reflect those most impacted by maternal health disparities and 2) direct pathway for a highly skilled and community-cultivated workforce necessary to sustain the MRHV program.
Mothers Rising Theory of Change
The theory of change for MRHV operationalizes the founders’ commitment to implementing a place-based approach that mobilizes a perinatal workforce deeply rooted in and dedicated to advancing the health and well-being of the community. This theory of change reflects the tenets of culture, social connection, and community care. It highlights four key components: rigorous training, cultural reflection, social proximity, and a three-generational approach (Figure 1).
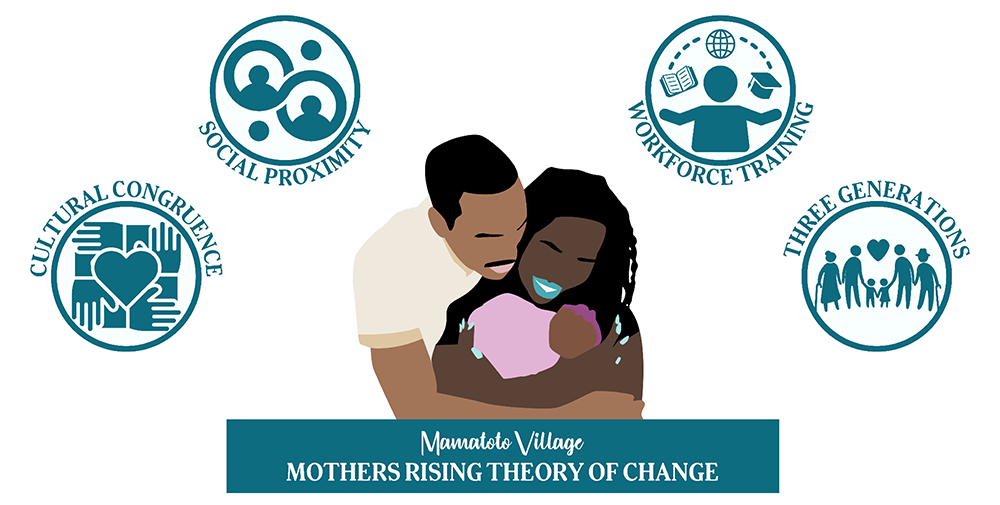
Training. As described above, women from the communities that the MRHV program serves are recruited to join a rigorous training cohort. With didactic education, MV’s workforce training is focused on the specialty of perinatal health infused in a CHW model grounded in human rights, reproductive, and birth justice.
Cultural reflection. The program approaches perinatal care through cultural congruence and humility. PHWs are highly trained professionals with direct ties to the community. They are dedicated to delivering respectful care that celebrates the participant’s culture. The Black experience is not a monolith; therefore, it is impossible to assume that the staff will reflect every aspect of the culture represented among clients. However, barriers to engagement are often overcome through a shared identification with Black culture. From interpersonal communication to educational materials, MRHV staff, administration, and clients are reflected throughout every aspect of the MRHV program, creating an environment of familiarity, safety, and trust.
Social proximity. The MV staff is comprised of people who mirror the experiences, family dynamics, and neighborhoods of those they serve. They strive to make the transition into parenthood self-determined and rooted in nurture, nonjudgmental support, advocacy, and evidence-based information, realizing their work impacts and uplifts the entire community. PCHWs are committed to meeting the needs of their clients where they are and providing services in various settings, including the home, providers’ offices, and the general community.
Three-generations approach. The mother-baby dyad does not exist in a silo. The recognition of the intergenerational transmission of health, health literacy, well-being, wealth, and social status is reflected in the three-generation approach, which is an upstream solution requiring holistic interventions to optimize parent and child bonding. It emphasizes the need to respectfully engage, educate, and empower the woman and the familial support system to move the entire family toward self-determination, wellness, and joy.
Essential Program Components
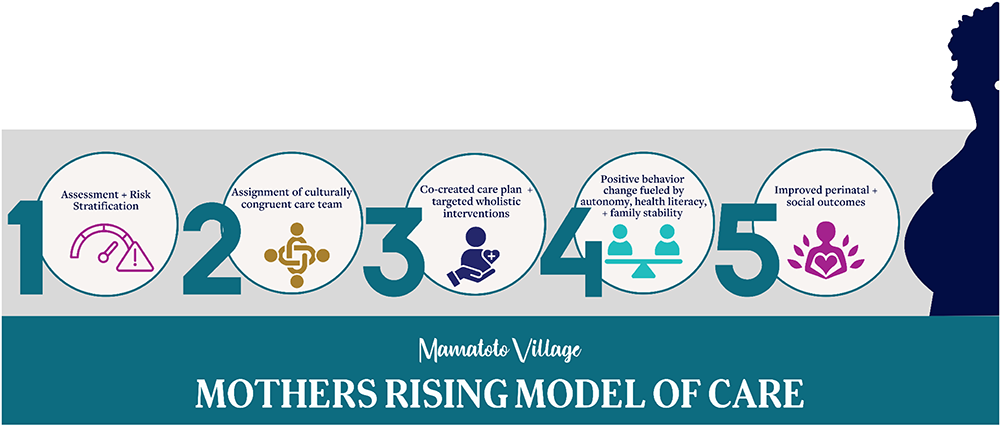
MRHV uses evidence-based and evidence-informed elements to form a core model with a cultural overlay that is adaptable and scalable for other communities, contexts, and populations. Over the span of an average 30-week enrollment, PHWs work in teams to provide clients with wrap-around care, including education and support related to pregnancy and postpartum, social needs, and overall wellness, including fitness, nutrition, stress management, mental health, and lactation. The building blocks for this approach are (1) an evidence-informed biopsychosocial intake assessment; (2) an interdisciplinary team-based model; (3) individualized care plans; (4) supported behavior change fueled by autonomy, health literacy, and family stability; and (5) improved perinatal and social outcomes (Figure 2).
Evidence-based Assessment
Upon referral to the MRHV program, clients complete a proprietary intake assessment. During this visit, clients self-report demographic information and detail their mental, physical, environmental, and social health. They also share their health status from preconception to the current pregnancy, as well as any past medical history. Following this assessment, clients are tiered using a perinatal risk stratification tool that combines health and social factors. This tool was adapted from the validated American Academy of Family Physicians’ Risk-Stratified Care Management and Coordination Tool (American Academy of Family Physicians, 2021).
Interdisciplinary Team-based Model
Care teams are comprised of a variety of Perinatal Health Workers (PHWs) who have expertise in one or several of the following areas: care coordination, perinatal education, nutrition and fitness, perinatal mental health and stress management, labor support, postpartum and newborn care, and lactation. Having a multidisciplinary team ensures clients receive specialized care tailored to their needs, while also ensuring each team member can perform duties within their area of expertise, while minimizing burnout.
Individualized Service Plans
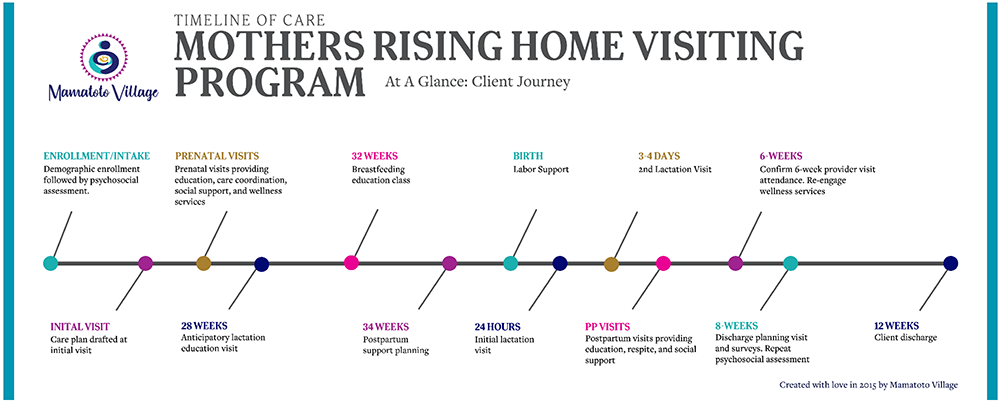
MRHV combines a standardized service schedule with customizable offerings to give each enrollee an individualized experience. Key services–such as antepartum and postpartum visits, breastfeeding anticipatory guidance, childbirth and parenting education, postpartum planning, and postpartum respite care–are offered to each participant on a standardized timeline (Figure 3). The cadence of visits is designed to align with the participant’s level of acuity and milestones in the perinatal period, where critical decision-making, education, and advocacy needs are elevated. Clients are also offered fundamental resources such as hygiene products, wellness supplies, baby care items, clothing, food, and safe sleep items.
Supported Behavior Change
During group sessions, clients are provided a safe space to build meaningful connections and a supportive community with other clients. These sessions facilitate social connection by uniting individuals around a shared goal of having a healthy pregnancy and positive parenting experience, creating an environment of mutual support and accountability. The sense of community helps normalize positive behavior changes, making healthy practices feel both achievable and socially reinforced. Sessions include perinatal fitness, childbirth education, newborn care, sudden infant death syndrome prevention, breastfeeding, perinatal mental health, and parenting skills. These classes and support groups focus on helping expecting parents maintain a healthy pregnancy and successful transition into parenthood by reducing pregnancy-related morbidities such as diabetes, hypertension, and preeclampsia, and educating them about childbirth, breastfeeding, and newborn care. Aside from coaching, classes, and support groups, MRHV offers access to necessary maternity and postpartum mother and child supplies, such as breastfeeding tools, clothes, and newborn essentials.
Improved Perinatal and Social Outcomes
The program collects, analyzes, and reports on program outcomes and impact using key perinatal indicators, including mode of delivery, gestational age, birthweight, breastfeeding initiation, and neonatal intensive care unit (NICU) admission status. Clients also self-report on employment, housing, food security, safety, and perceived stress indicators. Improvement of the participant’s socio-emotional stability is assessed by comparing data about these indicators collected at the start and end of program enrollment.
Building Evidence
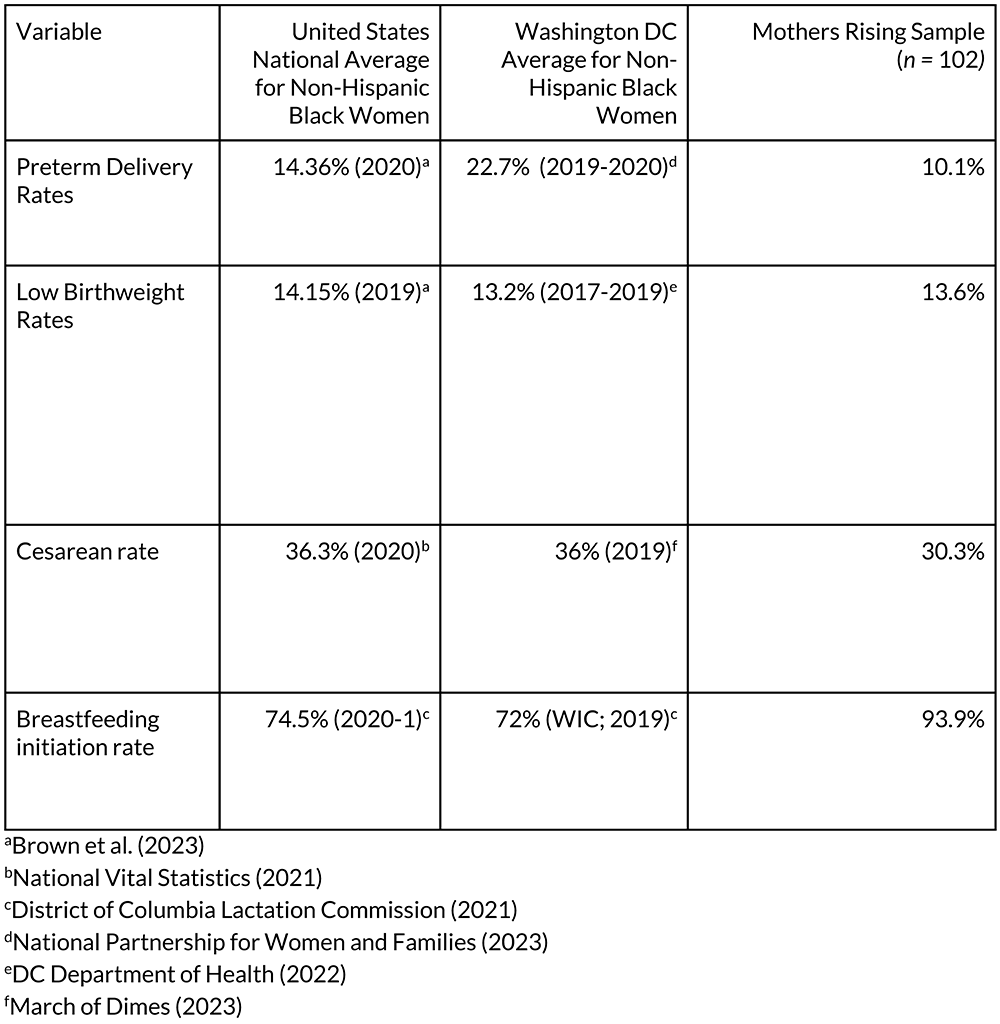
Since its founding, MV has been identified as a viable community-led solution to the Black maternal health crisis (Barthel et al., 2022; Goode, 2014; National Partnership for Women and Families, 2019). Recognized as an award-winning and cutting-edge practice by the Association of Maternal and Child Health Programs (AMCHP), MRHV has advanced health equity and improved maternal outcomes for historically marginalized perinatal populations over the past ten years. The program has provided service to over 2,000 Black women and supported more than 1,000 births while maintaining a 0% maternal mortality rate. In 2021, MV partnered with Georgetown University’s Center of Child and Human Development to conduct a mixed-methods evaluation of MRHV. Data from a sample of 102 participants were compared with a group of similar birthing people drawn from a Medicaid managed care organization serving Washington, DC. Small but statistically significant differences in gestational age favoring the MRHV participants were found (Snowden et al., 2024). Additional quantitative data demonstrating clinically significant differences in a broader range of perinatal outcomes are presented in Table 1.
Table 1. Quantitative Data Comparing Outcomes for Mothers Rising Home Visiting Participants and Non-participants in the United States and Washington DC.
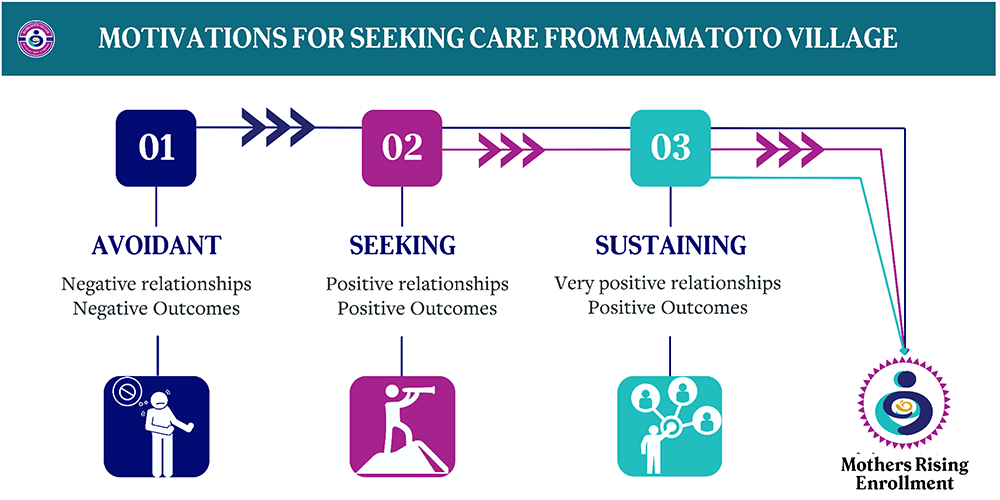
In addition to analyzing quantitative data, the evaluation team also interviewed 10 MRHV participants who had had a prior pregnancy without the support of the MRHV program, essentially serving as their own comparison group. The full results of these analyses will be published separately, but they provide additional support for the program’s theory of change. One example from the qualitative findings highlights participant motivations for seeking care from a community-led and rooted perinatal home visitation program. Participant motivations were coded into three categories: 1) avoidant: seeking to avoid recurrent negative experiences, 2) seeking: seeking to replicate the positive care experiences or relationships they previously experienced, and 3) sustaining: having a desire to deepen already established experiences in culturally reflective care (Figure 4). Regardless of their motivation for entry, the experience and support provided by the MRHV team were transformative. One participant stated, “Everybody was Black women, it’s Black women everywhere. [My PCHW], like she’s from DC, she lives in DC, so she understands the culture here and how we are here and things that may rub me the wrong way or may not… So, I really like that she understood me and who I was, and she had no problem coming to my house despite what goes on out there.”
Conclusion
Addressing the Black maternal health crisis requires more than clinical interventions; it demands culturally congruent, community-rooted models of care that are affirming, build trust, and acknowledge the lived realities of those most impacted. Mamatoto Village’s Mothers Rising Home Visiting (MRHV) program exemplifies what is possible when reproductive justice, cultural humility, and community leadership are central to care. Through rigorous workforce development, culturally reflective services, social connection, and an intergenerational approach, MRHV advances health equity and fosters community resilience. The program’s success, demonstrated by its positive perinatal outcomes, proves the value of investing in community-led solutions. Moreover, MRHV builds social capital by creating supportive networks that normalize positive behavior change and empower families to thrive. Mothers Rising Home Visiting offers a pathway, not only for the families of Washington, DC, but for communities across the country seeking to dismantle inequities and reimagine perinatal care through the lens of justice, joy, and self-determination.

Acknowledgments
All research activities were conducted in accordance with prevailing ethical principles. This study was reviewed and approved by the Georgetown University Institutional Review Board. The research team would like to extend deep gratitude to Cassietta Pringle, co-founder of Mamatoto Village, for her visionary leadership in establishing MV. Her insights and historical perspective were invaluable in understanding the origins and vision of the organization. The team would also like to honor the contributions of women, past and present, who have served and been served at Mamatoto Village. Their stories, labor, and resilience are the foundation and future of this work.
References
American Academy of Family Physicians. (2021, May 5). AAFP tools ease patient risk stratification, care planning. AAFP. https://www.aafp.org/news/practice-professional-issues/20210505rscmtools.html
Bakst, C., Moore, J. E., George, K. E., & Shea, K. (2020, May). Community-based maternal support services: The role of doulas and community health workers in Medicaid. Institute for Medicaid Innovation. https://medicaidinnovation.org/wp-content/uploads/2022/09/2020-IMI-Community_Based_Maternal_Support_Services-Report.pdf
Barthel, M., Dwyer, D., & Gomez, A. M. (2022, August 18). We want them to feel uplifted: This health clinic fills a gap in care for pregnant people in Wards 7 and 8. DCist. https://dcist.com/story/22/08/18/mamatoto-village-dc-black-maternal-health-ward-7-and-8/
Brown, C.C., Moore, J.E., & Tilford, J.M. (2023). Rates of preterm birth and low-birthweight: an analysis of racial and ethnic populations. Health Affairs, 42(2): 261-267. https://pmc.ncbi.nlm.nih.gov/articles/PMC10062121/
District of Columbia Department of Health. (2022). Perinatal health and infant mortality report 2019-2020. https://dchealth.dc.gov/sites/default/files/dc/sites/doh/publication/attachments/2022-07-CPPE-PHIMreport-9-web.pdf
District of Columbia Lactation Commission (2021). 2019-2020 Annual Report to Mayor Muriel Bowser. https://dchealth.dc.gov/sites/default/files/dc/sites/doh/service_content/attachments/Lactation%20Commission%202019-2020%20Report%20-%20FINAL.pdf
Goode, K. L. (2014). Birthing, blackness, and the body: Black midwives and experiential continuities of institutional racism. [Doctoral dissertation, The Graduate Center The City University of New York]. CUNY Academic Works.
Hoyert, D.L. (2023, March). Maternal mortality rates in the United States. Centers for Disease Control and Prevention, National Center for Health Statistics. https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2021/maternal-mortality-rates-2021.pdf
Julian, Z., Robles, D., Whetstone, S., Perrit, J. B., Jackson, A. V., Hardeman, R. R., Scott, K. A. (2020). Community-informed models of perinatal and reproductive health services provision: A justice-centered paradigm toward equity among Black birthing communities. Seminars in Perinatology, 44(5), 1-8. https://doi.org/10.1016/j.semperi.2020.151267
Kukla, R., & Wayne, K. (2016). Pregnancy, birth, and medicine. The Stanford encyclopedia of philosophy (Spring 2023 Edition), Zalta, E. N., & Nodelman, U. (eds.), https://plato.stanford.edu/archives/spr2023/entries/ethics-pregnancy/
Lett, E., Hyacinthe, M. F., Davis, D. A., & Scott, K. A. (2023). Community support persons and mitigating obstetric racism during childbirth. The Annals of Family Medicine, 21(3), 227-233. DOI https://doi.org/10.1370/afm.2958
March of Dimes (2023). Where you live matters: maternity care deserts and the crisi of access and equity. https://www.marchofdimes.org/peristats/assets/s3/reports/mcd/Maternity-Care-Report-DistrictofColumbia.pdf
Menzel, A. (2021). The midwife’s bag, or, the objects of Black infant mortality prevention. Journal of Women in Culture and Society, 46(2), 283-309. https://doi.org/10.1086/710806
National Partnership for Women and Families (2019). Tackling maternal health disparities: A look at four local organizations with innovative approaches. https://nationalpartnership.org/wp-content/uploads/2023/02/tackling-maternal-health-disparities-a-look-at-four-local-organizations-with-innovative-approaches.pdf
National Partnership for Women and Families (2023). Black women’s maternal health: A multifaceted approach to addressing persistent and dire health inequities. https://nationalpartnership.org/wp-content/uploads/black-womens-maternal-health.pdf
National Vital Statistics Reports. (March 23, 2021). Births: Final data for 2019. 70(2): 1-51.
Office of the Chief Medical Examiner (2021). Maternal Mortality Review Committee 2019-2020 annual report. Retrieved from https://ocme.dc.gov/sites/default/files/dc/sites/ocme/agency_content/Maternal%20Mortality%20Review%20Committee%20Annual%20Report_Finalv2.pdf
Oregon Health and Science University (n.d.). A brief history on midwifery in America. Center for Women’s Health. https://www.ohsu.edu/womens-health/brief-history-midwifery-america#:~:text=The%20decline%20in%20midwifery%2Dattended,in%20birth%20and%20reducing%20interventions.
Snowden, E., Perry, D. F., Amina, R., Shaw, B., & Nedhari, A. (2024). Assessing the impact of a culturally congruent perinatal home-visiting program on gestational age at delivery for Black women. Health Equity, 8(1), 599-607. DOI:10.1089/heq.2024.0076.
Authors
Snowden, Erin, MPH
Mamatoto Village,
4315 Sheriff Road NE, Washington, DC 20019 USA
erin@mamatotovillage.org
Nedhari, Aza, CPM, LPC
Mamatoto Village,
4315 Sheriff Road NE, Washington, DC 20019 USA
Perry, Deborah F., PhD
Georgetown University,
2115 Wisconsin Avenue NW, 6th Floor, Washington, DC 20007 USA
Amina, Rabiyah, MPP, MS
Mamatoto Village,
4315 Sheriff Road NE, Washington, DC 20019 USA





