
Abstract
In the field of infant and early childhood mental health (IECMH), there is a need for decolonized theories, research, community interventions, and clinical practice that are viewed through the lens of colonization and racism. This decolonization of reflective practice is a process that emphasizes the critical role of dynamic self-awareness for IECMH professionals serving targeted colonized and racially traumatized groups. This paper presents a process model of reflective practice based on foundational principles of the sociocultural and psychological impact of the shared trauma responses of slavery and colonization that manifest as hidden Adverse Childhood Experience (ACEs). The toxic behavioral outcomes of voicelessness, feelings of invisibility, unrecognized privileges and power, emotionless responses in relationships of the oppressed and oppressor, and reactive agency (VIPERs) are discussed within the framework. We offer a checklist as a tool to guide the decolonization of reflective practice in a relationship-based space for supervisor and practitioner. The paper concludes with a call to action for training local groups of IECMH professionals to collectively examine and develop tools based on local cultural beliefs, values, and norms within the communities they serve.
Keywords: Reflective Supervision, Infant Mental Health, Early Relational Health, Historical Trauma, Reflective Practice, Colonization, Anti-Racist, Power, Privilege, ACE Adverse Childhood Experience, Community Interventions, Culture, Race, Ethnicity, Internalized Oppression.
The Process of Decolonizing the Shared Space in Reflective Practitioner/Supervisor Relationships
Throughout history human development centered on the need for protective interpersonal relationships. Relationships among humans first ensured the simple survival of the group. The introduction of the concept of mental health introduced the dynamic quality of relationships that lead to human thriving. From the secure-base of attachment relationships to the confidential and trusted space of therapy in clinical practice, the quality of the relationship is the key outcome. When humans experience the threat of oppression in modern times the quality of relationships may be impacted, and revert to the early survival mode.
In the field of infant and early childhood mental health (IECMH), there is a need for theories, research, community interventions, and clinical practice that are viewed through the lens of colonization and racism. We need to confront the prevailing paradigm of human development based on Western, industrialized, educated, rich, democratic (WEIRD) societies (Henrich et al., 2010). This theoretical framework leads to a paradigm of relationships that center the individual socialized into standards and cultural prescriptions for behaviors grounded in Eurocentric values and perspectives. The act of decolonizing reflective practice within a framework of relationships presents a new direction for workforce initiatives to achieve goals of effective, supportive services to families from groups targeted for discrimination, racial trauma, and structural inequality. Reflective Supervision/Consultation (RSC) raises awareness of the implications of shared racialized trauma and the need for protection through anti-racist organizational strategies (Hardy & Bobes, 2017; Noroña et al., 2021; Shivers et al., 2022; Wilson & Barron, 2022).
Trauma reverberates throughout a social system and across generations (Lewis, 1996; Moore, et al., 2023; Perry, et al, 2021; van der Kolk, 2014). Decolonizing reflective practice requires a flexible process model that utilises an ecological systems theoretical framework which includes the individual, contextual, and sociocultural factors influencing the early relational health of infants and young children, family health, and community well-being (Lewis et al., 2021; Shivers et al., 2022). In a decolonizing process model of reflective practice, the first step is understanding that the trauma of oppression, colonization, and racism is a shared experience. Maria Sotero’s (2006) public health model of historical trauma provides a sound theoretical framework for this beginning point, noting that what is often missing in descriptions of historical trauma events, such as genocide, slavery, and wars, is the psychological reality that all members of the society are impacted. The legacies of these shared trauma responses are factors that shape the quality of relationships of members of the group targeted for the violence of oppression and members of the group carrying out the violence to oppress. Trauma responses amongst the targeted group, such as active or passive resistance, protective parenting responses from parents (Lewis, 2019), and, in extreme cases, internalized colonization (Fanon, 1968; Worrell et al., 2024), are the result of survival by any means necessary. In this psychological state, the targeted group may come to believe the toxic stereotypes about themselves and their group members. For members of the dominant oppressor group, their trauma response reflects experiences in a system designed to subjugate one population and assign dominance and power to another. These unearned privileges are translated into all the areas of the social determinants of health, most notably education, employment, and the criminal justice system.
The process of reflection on shared trauma begins with understanding the sociocultural meaning of “self and targeted others” identifying the “privileged self” and “subjugated self” (Hardy & Bobes, 2016; Lewis et al., 2023). Most importantly, the quality of dynamics in interpersonal relationships—specifically emotional tone, communication styles, and the dynamics of power—between members of the oppressed social class and the dominant oppressor group is central to the decolonization process.
We argue that decolonized reflective practice centers on the underrecognized childhood experience of race-based trauma of families and professionals that impact the quality of interpersonal relationships—that the context of race, power, and privilege is a ‘nappy-haired ghost in the nursery’ that must be acknowledged (Fraiberg, 1975; Lewis, et al., 2023). Whereas being ‘nappy-haired’ refers to African-Americans that have kinky, tightly coiled, and textured hair which leads to childhood experiences of racial acceptance or rejection (CERAR) (Lewis, 2021; Lewis et. al., 2021). We propose that the lived experiences of the historical traumas of colonization and slavery are the hidden Adverse Childhood Experiences (ACEs) that may emerge as trauma triggers in modern experiences of both sides of the relationship in reflective practice. These unrecognized implicit biases, discrimination, policies, and practices are based on stereotypes that support a social hierarchy for a racially and culturally specific “standard normal person” (Ossorio, 1995). Recognizing them endorses the process of decolonizing reflective practice through a developmental lens of shared traumas.
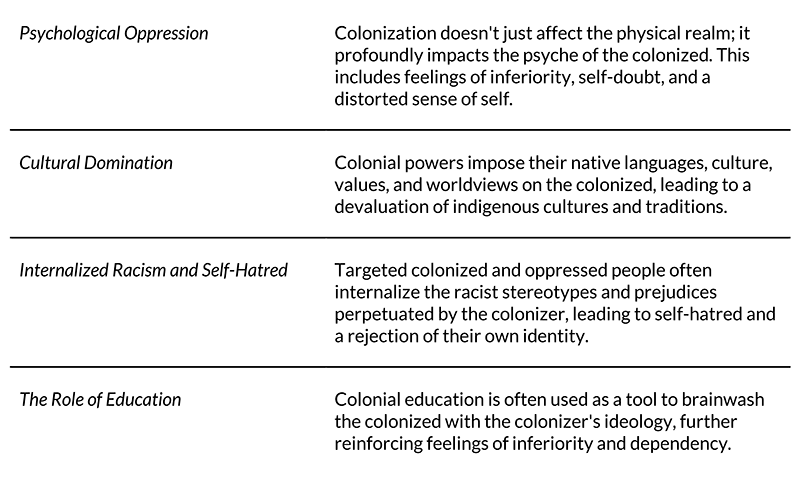
Table 1. Fanon’s (1968) Core Principles of Internalized Colonization.
The Process Model of Decolonized Reflective Practice
True liberation necessitates both political independence and a comprehensive psychological and cultural decolonization process (Moore et al., 2023; Wilkenson, 2020). Table 1 presents the psychological outcomes to colonized groups in the bottom rungs of social hierarchies. Decolonized reflection is an honest appraisal of individual responses to the psychologically toxic social context of systemic racism, structural inequality, and oppression. The racialized trauma responses may include, voicelessness, invisibility, unrecognized privileges and power, emotionlessness, and reactive agency – VIPER – experienced by both members of the targeted oppressed groups and members and descendants of the groups that oppressed them. Intentional strategies are necessary to recognize and disrupt the traumatic and poisonous outcomes of VIPERs in a decolonized reflective practice relationship.
Voicelessness as a shared trauma response refers to the systematic silencing and suppression of a group’s narratives, experiences, and perspectives (Duran & Duran, 2000). For oppressed, marginalized cultural, racial, or religious groups, this coping behavior often manifests as an internalized inability or unwillingness to speak out against injustice, share their suffering, or advocate for their rights due to generations of being ignored, dismissed, or punished. This act of self-silencing is a survival mechanism aimed at preventing further harm or re-traumatization. Still, it can lead to a profound sense of powerlessness and a culture of silence where individuals may avoid discussing traumatic pasts or present-day grievances, even within their own families and communities.
To be invisibilized means that the existence, contributions, suffering, and cultural practices of a group are systematically erased from the historical record (Fanon, 2008; Wilkenson, 2020). As an invisibilized group, subsequent generations are also ignored, denied, or rendered invisible within the dominant societal narrative. In response to colonization and oppression, marginalized groups may cope by adopting behaviors that further their invisibility, such as withdrawing from mainstream society, minimizing their cultural markers, or suppressing their unique identities to avoid discrimination or persecution. These coping mechanisms can protect individuals from direct harm or scrutiny, but also perpetuate their marginalization by denying them recognition, resources, and a place in collective memory (Fan & Ma, 2014).
In response to the unrecognized privileges and power in societies of structural inequality, the dominant group often responds with a range of behaviors that serve to maintain the status quo (Wilkenson, 2020). These responses frequently stem from a lack of awareness, an inability to critically examine their position, or as a defense mechanism against perceived threats to their advantages. Typical responses include dismissing the existence of systemic inequalities or attributing disparities to individual failings rather than structural issues, minimizing the impact of historical trauma or ongoing discrimination on marginalized groups, defensiveness and feelings of being personally blamed or attacked, and anger or resentment when privileges are pointed out. The oppressor may also engage in color-blindness or claiming not to “see” race or other social categories, which, while seemingly benevolent, effectively ignores the realities of systemic discrimination and the unique experiences of marginalized groups (McIntosh, 1988). The prism of unacknowledged privilege often results in a lack of accountability for the historical and ongoing perpetuation of inequalities and a resistance to policies or actions that aim to address these imbalances. Ultimately, the unrecognized nature of privilege enables the dominant group to maintain its elevated position without acknowledging the historical and ongoing mechanisms that sustain it, thereby perpetuating structural inequality (Lewis et al., 2023).
Emotionless behavior, in the context of historical trauma, describes a coping mechanism where individuals or groups appear to suppress, numb, or detach from their emotions. This is not a genuine absence of emotion, but rather a protective strategy to manage overwhelming pain, grief, or anger stemming from past and ongoing oppression, avoid re-experiencing intense emotional distress, or present an impenetrable façade to the dominant group (Stuckey, 1987). The classic poem of Paul Laurence Dunbar (1997) “We Wear the Mask,” describes the necessity for marginalized people, specifically African Americans, to “mask,” hiding their true emotions behind a façade of smiles and pleasantries as a “debt [paid] to human guile” that allows individuals to survive.
Reactive-agency refers to how oppressed and marginalized groups assert their will and agency in response to the historical traumas and ongoing injustices they face. Unlike proactive agency which involves initiating change from a position of power, (Bandura, 1997), reactive agency often responds to existing oppressive structures or events. This reactive response to chronic experiences of racial trauma can manifest as acts of resistance, protest, cultural preservation, community organizing, or the development of unique coping strategies that challenge dominant narratives and reclaim identity. For example, the creation of distinct cultural practices, languages, or spiritual beliefs can be an act of reactive agency, preserving a sense of self and community in the face of attempts to erase them (Moore et al., 2023; Stuckey, 1987). It signifies a refusal to be wholly defined or defeated by trauma, even if the actions are primarily in response to external pressures rather than initiated from a position of complete autonomy (Fine & Weis, 1998).
Table 2. VIPER: A Tool for Decolonizing Relationships for Authentic Reflective Practice.

Guidelines for the process of development of a decolonized IECMH training
IECMH professionals working on behalf of targeted colonized and racially traumatized groups may benefit from receiving professional development from IECMH professionals that engage in decolonized reflective practice. This can be one anti-racist tool to eradicate the VIPERs in the interpersonal relationships between IECMH professionals and the infants, children, and families they serve.
The authors engaged in this process from 2019 to 2022 in a northeast American city with significant racial disparities in child health and wellbeing, educational outcomes, economic wellbeing, and housing (ACT Rochester, 2020). This imperfect initial attempt can serve as a guideline for what is possible when it comes to available tools to decolonize IECMH training and ensure better outcomes for diverse families and communities (Lewis et al., 2023). We recommend embarking on the following steps in conjunction with the Alliance for the Advancement of Infant Mental Health’s Training Guide & Self Assessment.
- Gather a diverse training staff with unique perspectives and ways of knowing. Ideal candidates may not be content experts at first glance, but consider the wealth of experience that parents of children with disabilities, the neighborhood elder, a community organizer, a retired educator, or clergy member might offer. It’s easier to teach someone how to deliver a training than it is to teach human connection, resilience, and relationship-based values. If a scan of your community fails to produce what you’re looking for, turn to your stakeholders. Ask early care and education directors, pre-k teachers, families receiving community-based services, or home visiting staff who they would recommend to help other professionals best learn about decolonized early relational health.
- Recognize any limitations of knowledge on the subject regardless of your experience, education, and expertise. When you know—and acknowledge—what you don’t know, you can call in other perspectives to fill those gaps and provide feedback (e.g., parent leaders, former clients, etc.).
- Model parallel process by cultivating a relationship with a reflective consultant steeped in decolonizing reflective practice. A consultant can provide direct and indirect training development support throughout the process as well as a holding container for the trainers to grow and thrive. When IECMH trainers receive decolonized reflective practice support, they are more resourced and empowered to provide it to others.
- When engaging in the parallel process of receiving decolonized reflective practice support, ensure staff from targeted colonized and racially traumatized groups receive support from someone who shares that identity. If this is not available or not an option, provide existing reflective supervisors with robust training, education, and relationship-based support specific to racialized reflective practice. Operate under the assumption that they have the capacity to cause harm and supervisees may be afraid to fully express themselves. Familiarize yourself with the Digging Deeper Report: Decolonizing our Understanding and Practice of Reflective Supervision through a Racial Equity Lens (Shiver et al., 2022).
- Resist the urge of White Supremacy Culture to get this done quickly. Once the team is gathered and receiving decolonized support, you may need to meet regularly over many months to develop a consensus on gaps in knowledge, build relationships, and collect multiple perspectives. The authentic implementation of decolonization in reflective practitioner/supervisor relationships is a journey (Lewis et al., 2023).
- Set initial parameters on what must be covered during training and then unleash your trusted team on curriculum development. Example of parameters include:
- Identifying ways to uplift diverse voices, particularly of Black, Indigenous, and People of Color (BIPOC) IECMH experts
- Providing multiple ways of learning/engaging in the content (e.g., internal reflection, external expression, opportunities for individual and group creativity, hands-on practice, etc.).
- Resist primarily didactic ways of educating and instead be curious about how to engage adult learners in unique ways. Can you be more playful, prioritize discussion over lecture, or forego a PowerPoint altogether?
- Including diverse images, voices, and examples of parenting people in training content to ensure diverse participants can see themselves reflected.
- Remain curious and test out materials with training cohorts to adapt them based on feedback and new information. Explore the following questions with your team to reflect back on the process and consider your next steps:
- What was most supportive in decolonizing our IECMH training?
- What might you need more of to sustain this work?
- Which relationships forged during the training will stick with you?
- Share something you learned that you want to integrate into the next offering.
- Explore themes from the VIPER model (e.g., How did we address voicelessness or emotionlessness in our training cohort? How did we keep privilege and power in mind?)
- Provide payment for services for any person assisting with the development, delivery, or consultation of this training for decolonized reflective supervision or practice.
Conclusion
The process of building authentic relationships between people from the oppressed and oppressor groups offers a clear ray of hope and healing. To support decolonized reflective practice, there is a critical need for tools and relationship-based strategies that elevate traditional cultural practices, leading to collective survival and thriving.
References
ACT Rochester. (2020). Hard facts update: Race & ethnicity in the nine-county greater Rochester area. The Rochester Area Community Foundation. https://www.actrochester.org/all-reports/hard-facts-update-2020
Alliance for the Advancement of Infant Mental Health. (n.d.). Preparing competency-based learning for infant and early childhood mental health endorsement: Training guide and self-assessment. https://www.allianceaimh.org/trainingguideandselfassessment
Bandura, A. (1997). Self-efficacy: The exercise of control. W.H. Freeman and Company.
Dunbar, P. L. (1997). We wear the mask. In J. R. Sherman (Ed.), African-American poetry: An anthology, 1773–1927 (p. 29). Dover Thrift Editions.
Duran, E., & Duran, B. (2000). Native American postcolonial psychology. State University of New York Press.
Fan, S., & Ma, Y. (2014). Invisibilized: How Chinese women in diaspora experience and cope with racism in the United States. Journal of International and Intercultural Communication, 7(2), 154-172.
Fanon, F. (2008). Black skin, white masks. Grove Press.
Fine, M., & Weis, L. (1998). The unknown city: Lives of poor and working-class young adults. Beacon Press.
Fraiberg, S., Adelson, E., & Shapiro, V. (1975) Ghosts in the nursery: A psychoanalytic approach to the problems of impaired infant-mother relationships. Journal of American Academy of Child Psychiatry, 14(3), 387-421. https://doi.org/10.1016/S0002-7138(09)61442-4
Hardy, K. V., & Bobes, T. (Eds.). (2016). Culturally sensitive supervision and training: Diverse perspectives and practical applications. Routledge.
Hardy, K. V., & Bobes, T. (2017). Promoting cultural sensitivity in supervision: A manual for practitioners. Routledge.
Henrich, J., Heine, S. J., & Norenzayan, A. (2010). The weirdest people in the world? Behavioral and Brain Sciences, 33(2-3), 61-83.
Lewis, M. L. (1996). Trauma reverberates: Psychosocial evaluation of the caregiving environment of young children exposed to violence and traumatic loss. Island of safety: Assessing and treating young victims of violence (Vol. 16, pp. 21-28). ZERO TO THREE Publications.
Lewis, M. L. (2019). The intergenerational transmission of protective parenting responses to historical trauma. In H. E. Fitzgerald, D. Johnson, D. Qin, F. Villarruel, and J. Norder (Eds.). The Handbook of Children and Prejudice: Integrating Research Practice and Policy, 43-61. Springer Publishers. https://doi.org/10.1007/978-3-030-12228-7
Lewis, M. L. (2021). Childhood experiences of racial acceptance and rejection. In M. L. Lewis & D. J. Weatherston (Eds.), Therapeutic cultural routines to build family relationships: Talk, Touch & Listen While Combing Hair© (pp. 3–17). Springer Nature Switzerland AG. https://doi.org/10.1007/978-3-030-83726-6_1
Lewis, M. L., Dunjwa, M., & Cohen, C. (2021). Guidelines to identify child-endangering hair styling practices: Medical, legal, and psychosocial perspectives. In M. L. Lewis & D. J. Weatherston (Eds.), Therapeutic cultural routines to build family relationships: Talk, Touch & Listen While Combing Hair© (pp. 3–17). Springer Nature Switzerland AG. https://doi.org/10.1007/978-3-030-83726-6_1
Lewis, M. L., & Weatherston, D. (Eds.). (2021) Therapeutic cultural routines to build family relationships. Talk, touch, and listen while combing hairⒸ. Springer Publishers. https://doi.org/10.1007/978-3-030-83726-6
Lewis, M. L., Colson, S., Durlak, L., & Smith, M. (2023). Reflective practice through a racialized lens: My hero’s journey. Archway Publishers.
McIntosh, P. (1989). White privilege: Unpacking the invisible knapsack. National SEED Project.
Moore, E., Irving, D., Penick-Parks, M., & Fox Tree C. A. (2023). 21-Day Racial Equity Indigenous challenge fighting white supremacy since 1492. https://www.americaandmoore.com/21-day-indigenous
Noroña, C. R., Lakatos, P. P., Wise-Kriplani, M., & Williams, M. E. (2021). Critical self-reflection and diversity-informed reflective supervision/consultation. ZERO TO THREE, December 2021, 62-71.
Ossorio, P. G. (1995). Persons (Vol. I). Descriptive Psychology Press.
Perry, B. D., & Winfrey, O. (2021). What happened to you?: Conversations on trauma, resilience, and healing. Flatiron Books.
Shivers, E. M., Janssen, J. A., Subramaniam, A., Parker, A. L., Noroña, C. R., Lara, C., Best, D., Yazzie, D. A., Cimino, J., Kohchi, J., Fitzgibbons, S. (2022). Digging deeper: De-colonizing our understanding and practice of reflective supervision through a racial equity lens. Prepared by Indigo Cultural Center for the Alliance for the Advancement of Infant Mental Health with funding from Perigee Fund.
Sotero, M. M. (2006). A conceptual model of historical trauma: implications for public health, practice and research. Journal of Health Disparities Research and Practice (1)1:93-108.
Stuckey, S. (1987). Slave culture: Nationalist theory and the foundations of Black America. Oxford University Press
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Viking.
Wilson, K. A.. & Barron, C. C. (2022). Honoring race and diversity in reflective supervision: Guiding principles to enhance relationships. Zero to Three Journal, 42(4), 14-20.
Wilson, K. A., Weatherston, D. J., & Hill, S. (2021). Introduction to reflective supervision: Through the Lens of culture, diversity, equity, and inclusion. In M. L. Lewis & D. J. Weatherston, (Eds.). Therapeutic cultural routines to build family relationships. Talk, touch, and listen while combing hairⒸ. (pp. 75-84). Springer Publishers. https://doi.org/10.1007/978-3-030-83726-6
Wilkerson, I. (2020). Caste: The origins of our discontents. Allen Lane.
Worrell, F. C., Vandiver, B. J., & Fhagen, P. E. (2023). Nigrescence theory from 1971 to 2021: The critical contributions of William E. Cross, Jr. American Psychologist, 78(4), 389–400. https://doi.org/10.1037/amp0001052
Authors
Lewis, Marva L.
Department of Psychiatry and Neurology, Tulane University School of Medicine; Tulane University School of Social Work,
United States
Smith, Megan M.
Nazareth University School of Education and College of Health and Human Services,
United States
Correspondence concerning this article should be addressed to Marva L. Lewis, mlewis@tulane.edu





